
Page 370 - Basic _ Clinical Pharmacology ( PDFDrive )
P. 370
356 SECTION IV Drugs with Important Actions on Smooth Muscle
but inhibit both antigen- and exercise-induced bronchospasm in OCH
asthmatic patients. 3
O H
O
O O O N O
S NH
–
Na + – OC O O CO Na + O
CH 3 N
OH
CH 3
O OCH CHCH O O Zafirlukast
2
2
Cromolyn sodium
–
COO Na +
S
O H CCH 2 CH CH CH 3 O
2
2
3
Cl
–
Na + – OC N O CO Na + N
HO
H C
3
H C
3
O O Montelukast
Nedocromil sodium
CH 3 O
S
When taken regularly (2–4 puffs 2–4 times daily), these agents CH N C NH
modestly but significantly reduce symptomatic severity and 2
the need for bronchodilator medications, particularly in young OH
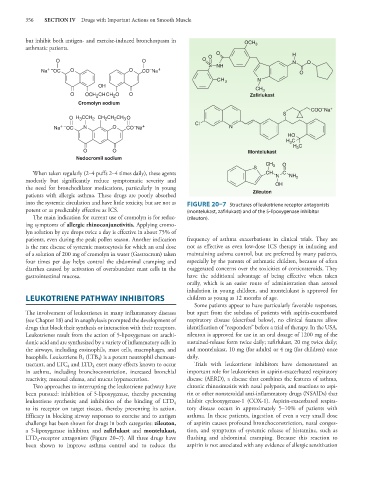
patients with allergic asthma. These drugs are poorly absorbed Zileuton
into the systemic circulation and have little toxicity, but are not as FIGURE 20–7 Structures of leukotriene receptor antagonists
potent or as predictably effective as ICS. (montelukast, zafirlukast) and of the 5-lipoxygenase inhibitor
The main indication for current use of cromolyn is for reduc- (zileuton).
ing symptoms of allergic rhinoconjunctivitis. Applying cromo-
lyn solution by eye drops twice a day is effective in about 75% of
patients, even during the peak pollen season. Another indication frequency of asthma exacerbations in clinical trials. They are
is the rare disease of systemic mastocytosis for which an oral dose not as effective as even low-dose ICS therapy in inducing and
of a solution of 200 mg of cromolyn in water (Gastrocrom) taken maintaining asthma control, but are preferred by many patients,
four times per day helps control the abdominal cramping and especially by the parents of asthmatic children, because of often
diarrhea caused by activation of overabundant mast cells in the exaggerated concerns over the toxicities of corticosteroids. They
gastrointestinal mucosa. have the additional advantage of being effective when taken
orally, which is an easier route of administration than aerosol
inhalation in young children, and montelukast is approved for
LEUKOTRIENE PATHWAY INHIBITORS children as young as 12 months of age.
Some patients appear to have particularly favorable responses,
The involvement of leukotrienes in many inflammatory diseases but apart from the subclass of patients with aspirin-exacerbated
(see Chapter 18) and in anaphylaxis prompted the development of respiratory disease (described below), no clinical features allow
drugs that block their synthesis or interaction with their receptors. identification of “responders” before a trial of therapy. In the USA,
Leukotrienes result from the action of 5-lipoxygenase on arachi- zileuton is approved for use in an oral dosage of 1200 mg of the
donic acid and are synthesized by a variety of inflammatory cells in sustained-release form twice daily; zafirlukast, 20 mg twice daily;
the airways, including eosinophils, mast cells, macrophages, and and montelukast, 10 mg (for adults) or 4 mg (for children) once
basophils. Leukotriene B (LTB ) is a potent neutrophil chemoat- daily.
4
4
tractant, and LTC and LTD exert many effects known to occur Trials with leukotriene inhibitors have demonstrated an
4
4
in asthma, including bronchoconstriction, increased bronchial important role for leukotrienes in aspirin-exacerbated respiratory
reactivity, mucosal edema, and mucus hypersecretion. disease (AERD), a disease that combines the features of asthma,
Two approaches to interrupting the leukotriene pathway have chronic rhinosinusitis with nasal polyposis, and reactions to aspi-
been pursued: inhibition of 5-lipoxygenase, thereby preventing rin or other nonsteroidal anti-inflammatory drugs (NSAIDs) that
leukotriene synthesis; and inhibition of the binding of LTD inhibit cyclooxygenase-1 (COX-1). Aspirin-exacerbated respira-
4
to its receptor on target tissues, thereby preventing its action. tory disease occurs in approximately 5–10% of patients with
Efficacy in blocking airway responses to exercise and to antigen asthma. In these patients, ingestion of even a very small dose
challenge has been shown for drugs in both categories: zileuton, of aspirin causes profound bronchoconstriction, nasal conges-
a 5-lipoxygenase inhibitor, and zafirlukast and montelukast, tion, and symptoms of systemic release of histamine, such as
LTD -receptor antagonists (Figure 20–7). All three drugs have flushing and abdominal cramping. Because this reaction to
4
been shown to improve asthma control and to reduce the aspirin is not associated with any evidence of allergic sensitization