
Page 658 - Basic _ Clinical Pharmacology ( PDFDrive )
P. 658
644 SECTION VI Drugs Used to Treat Diseases of the Blood, Inflammation, & Gout
Propionic acid derivative Pyrrolealkanoic acid derivative Phenylalkanoic acid derivative
COOH O CH 3 COOH COOH
C H C N CH 2
H C CH
3
CH CH 2 CH 3 CH 3
H C H C F
3
3
Ibuprofen Tolmetin Flurbiprofen
Indole derivative Pyrazolone derivative Phenylacetic acid derivative
COOH
H C O CH 2 CH COOH CI
3
2
N CH 3 N N NH
O O
C O
CI
CH 2 CH 2 CH 2 CH 3
CI
Indomethacin Phenylbutazone Diclofenac
Fenamate Oxicam Naphthylacetic acid prodrug
COOH
HO O O
N H C NH CH CH CCH
N 2 2 3
Cl Cl
N
S CH 3 H C O
3
CH 3 O O
Meclofenamic acid Piroxicam Nabumetone
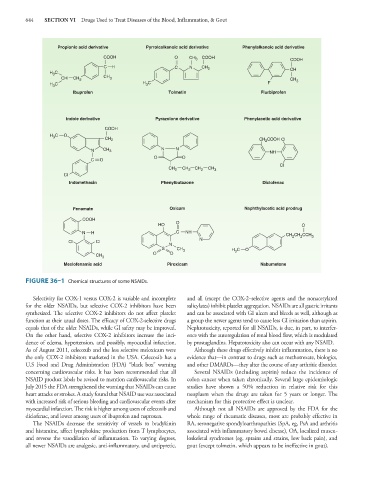
FIGURE 36–1 Chemical structures of some NSAIDs.
Selectivity for COX-1 versus COX-2 is variable and incomplete and all (except the COX-2–selective agents and the nonacetylated
for the older NSAIDs, but selective COX-2 inhibitors have been salicylates) inhibit platelet aggregation. NSAIDs are all gastric irritants
synthesized. The selective COX-2 inhibitors do not affect platelet and can be associated with GI ulcers and bleeds as well, although as
function at their usual doses. The efficacy of COX-2-selective drugs a group the newer agents tend to cause less GI irritation than aspirin.
equals that of the older NSAIDs, while GI safety may be improved. Nephrotoxicity, reported for all NSAIDs, is due, in part, to interfer-
On the other hand, selective COX-2 inhibitors increase the inci- ence with the autoregulation of renal blood flow, which is modulated
dence of edema, hypertension, and possibly, myocardial infarction. by prostaglandins. Hepatotoxicity also can occur with any NSAID.
As of August 2011, celecoxib and the less selective meloxicam were Although these drugs effectively inhibit inflammation, there is no
the only COX-2 inhibitors marketed in the USA. Celecoxib has a evidence that—in contrast to drugs such as methotrexate, biologics,
U.S Food and Drug Administration (FDA) “black box” warning and other DMARDs—they alter the course of any arthritic disorder.
concerning cardiovascular risks. It has been recommended that all Several NSAIDs (including aspirin) reduce the incidence of
NSAID product labels be revised to mention cardiovascular risks. In colon cancer when taken chronically. Several large epidemiologic
July 2015 the FDA strengthened the warning that NSAIDs can cause studies have shown a 50% reduction in relative risk for this
heart attacks or strokes. A study found that NSAID use was associated neoplasm when the drugs are taken for 5 years or longer. The
with increased risk of serious bleeding and cardiovascular events after mechanism for this protective effect is unclear.
myocardial infarction. The risk is higher among users of celecoxib and Although not all NSAIDs are approved by the FDA for the
diclofenac, and lower among users of ibuprofen and naproxen. whole range of rheumatic diseases, most are probably effective in
The NSAIDs decrease the sensitivity of vessels to bradykinin RA, seronegative spondyloarthropathies (SpA, eg, PsA and arthritis
and histamine, affect lymphokine production from T lymphocytes, associated with inflammatory bowel disease), OA, localized muscu-
and reverse the vasodilation of inflammation. To varying degrees, loskeletal syndromes (eg, sprains and strains, low back pain), and
all newer NSAIDs are analgesic, anti-inflammatory, and antipyretic, gout (except tolmetin, which appears to be ineffective in gout).