
Page 56 - SAMPLE
P. 56
3/7/2017 MonthlyCostChart
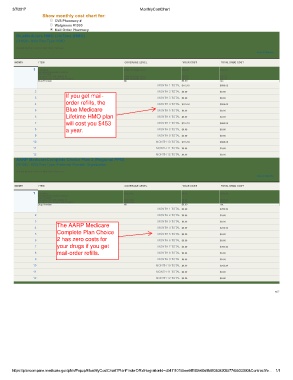
Show monthly cost chart for:
M o n th ly C o s t C h a rt
CVS Pharmacy #
Walgreens #1990
Mail Order Pharmacy
BlueMedicare HMO LifeTime (HMO)
(H1026 040) Plan Type: HMO
Detailed Monthly costs for Mail Order Pharmacy
View All Months
MONTH ITEM COVERAGE LEVEL YOUR COST TOTAL DRUG COST
1 Amlodipine Initial Coverage Level $39.00 $462.57
Besylate/Atorvastatin Calcium
TAB 1020MG
Bupropion Hcl TAB 300MG XL Initial Coverage Level $39.00 $60.27
Levothyroxine Sodium TAB 100MCG Initial Coverage Level $35.18 $35.18
Drug Premium NA $0.00 n/a
MONTH 1 TOTAL $113.18 $558.02
2 MONTH 2 TOTAL $0.00 $0.00
If you get mail-
3 MONTH 3 TOTAL $0.00 $0.00
order refills, the
4 MONTH 4 TOTAL $113.18 $558.02
5 Blue Medicare MONTH 5 TOTAL $0.00 $0.00
6 Lifetime HMO plan MONTH 6 TOTAL $0.00 $0.00
7 will cost you $453 MONTH 7 TOTAL $113.18 $558.02
8 MONTH 8 TOTAL $0.00 $0.00
a year.
9 MONTH 9 TOTAL $0.00 $0.00
10 MONTH 10 TOTAL $113.18 $558.02
11 MONTH 11 TOTAL $0.00 $0.00
12 MONTH 12 TOTAL $0.00 $0.00
AARP MedicareComplete Choice Plan 2 (Regional PPO)
(R7444 003) Plan Type: Preferred Provider Organization
Detailed Monthly costs for Mail Order Pharmacy
View All Months
MONTH ITEM COVERAGE LEVEL YOUR COST TOTAL DRUG COST
1 Amlodipine Deductible $0.00 $590.84
Besylate/Atorvastatin Calcium
TAB 1020MG
Bupropion Hcl TAB 300MG XL Deductible $0.00 $155.86
Levothyroxine Sodium TAB 100MCG Deductible $0.00 $35.84
Drug Premium NA $0.00 n/a
MONTH 1 TOTAL $0.00 $782.54
2 MONTH 2 TOTAL $0.00 $0.00
3 MONTH 3 TOTAL $0.00 $0.00
The AARP Medicare
4 MONTH 4 TOTAL $0.00 $782.54
Complete Plan Choice
5 MONTH 5 TOTAL $0.00 $0.00
6 2 has zero costs for MONTH 6 TOTAL $0.00 $0.00
7 your drugs if you get MONTH 7 TOTAL $0.00 $782.54
8 mail-order refills. MONTH 8 TOTAL $0.00 $0.00
9 MONTH 9 TOTAL $0.00 $0.00
10 MONTH 10 TOTAL $0.00 $782.54
11 MONTH 11 TOTAL $0.00 $0.00
12 MONTH 12 TOTAL $0.00 $0.00
w07
https://plancompare.medicare.gov/pfdn/Popup/MonthlyCostChart?PlanFinderDRxIntegrationId=d541110155ee44f182e60a9b89383420857745533390&ContractYe… 1/1