
Page 72 - Cover Letter & Evaluation for Isaac Kapon
P. 72
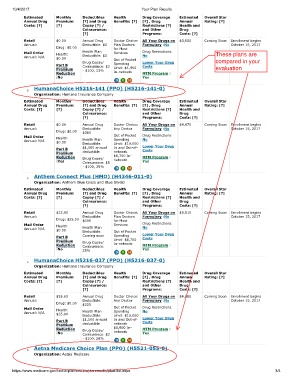
10/4/2017 Your Plan Results
Estimated Monthly Deductibles Health Drug Coverage Estimated Overall Star
Annual Drug Premium: [?] and Drug Benefits: [?] [?] , Drug Annual Rating: [?]
Costs: [?] [?] Copay [?] / Restrictions [?] Health and
Coinsurance: and Other Drug
[?] Programs: Costs: [?]
Retail $0.00 Annual Drug Doctor Choice: All Your Drugs on $3,550 Coming Soon Enrollment begins
Annual: Deductible: $0 Plan Doctors Formulary :No October 15, 2017
Drug: $0.00 for Most
Mail Order Health: Health Plan Services Drug Restrictions: These plans are
Annual: N/A $0.00 Deductible: $0 Out of Pocket No
Drug Copay/ Spending Lower Your Drug compared in your
Part B Coinsurance: $2 Costs
Premium - $100, 33% Limit: $1,900 evaluation
Reduction In-network MTM Program :
:No Yes
HumanaChoice H5216-141 (PPO) (H5216-141-0)
Organization: Humana Insurance Company
Estimated Monthly Deductibles Health Drug Coverage Estimated Overall Star
Annual Drug Premium: [?] and Drug Benefits: [?] [?] , Drug Annual Rating: [?]
Costs: [?] [?] Copay [?] / Restrictions [?] Health and
Coinsurance: and Other Drug
[?] Programs: Costs: [?]
Retail $0.00 Annual Drug Doctor Choice: All Your Drugs on $4,970 Coming Soon Enrollment begins
Annual: Deductible: Any Doctor Formulary :No October 15, 2017
Drug: $0.00 $365
Mail Order Health: Out of Pocket Drug Restrictions:
Annual: N/A $0.00 Health Plan Spending No
Limit: $10,000
Deductible:
Part B $1,500 annual In and Out-of- Lower Your Drug
Costs
Premium deductible network
Reduction Drug Copay/ $6,700 In- MTM Program :
:Yes Coinsurance: $5 network Yes
- $100, 25%
Anthem Connect Plus (HMO) (H4346-011-0)
Organization: Anthem Blue Cross and Blue Shield
Estimated Monthly Deductibles Health Drug Coverage Estimated Overall Star
Annual Drug Premium: [?] and Drug Benefits: [?] [?] , Drug Annual Rating: [?]
Costs: [?] [?] Copay [?] / Restrictions [?] Health and
Coinsurance: and Other Drug
[?] Programs: Costs: [?]
Retail $25.00 Annual Drug Doctor Choice: All Your Drugs on $5,510 Coming Soon Enrollment begins
Annual: Deductible: Plan Doctors Formulary :No October 15, 2017
Drug: $25.00 $405 for Most
Mail Order Health: Services Drug Restrictions:
Annual: N/A $0.00 Health Plan Out of Pocket No
Deductible:
Part B Coming soon Spending Lower Your Drug
Costs
Premium Drug Copay/ Limit: $6,700
Reduction Coinsurance: In-network MTM Program :
:No 25% Yes
HumanaChoice H5216-037 (PPO) (H5216-037-0)
Organization: Humana Insurance Company
Estimated Monthly Deductibles Health Drug Coverage Estimated Overall Star
Annual Drug Premium: [?] and Drug Benefits: [?] [?] , Drug Annual Rating: [?]
Costs: [?] [?] Copay [?] / Restrictions [?] Health and
Coinsurance: and Other Drug
[?] Programs: Costs: [?]
Retail $35.00 Annual Drug Doctor Choice: All Your Drugs on $4,880 Coming Soon Enrollment begins
Annual: Deductible: Any Doctor Formulary :No October 15, 2017
Drug: $0.00 $225
Mail Order Health: Out of Pocket Drug Restrictions:
Annual: N/A $35.00 Health Plan Spending No
Deductible:
Limit: $10,000
Part B $1,500 annual In and Out-of- Lower Your Drug
Costs
Premium deductible network
Reduction Drug Copay/ $5,900 In- MTM Program :
:No Coinsurance: $2 network Yes
- $100, 28%
Aetna Medicare Choice Plan (PPO) (H5521-055-0)
Organization: Aetna Medicare
https://www.medicare.gov/find-a-plan/results/planresults/plan-list.aspx 3/4