
Page 79 - Cover Letter & Evaluation for Isaac Kapon
P. 79
10/5/2017 Your Medicare Health Plan Details
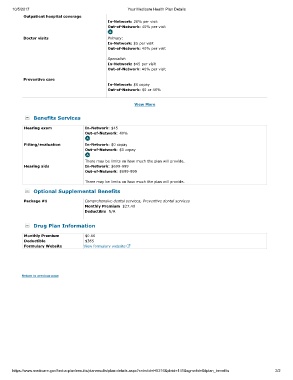
Outpatient hospital coverage
In-Network: 20% per visit
Out-of-Network: 40% per visit
Doctor visits Primary:
In-Network: $5 per visit
Out-of-Network: 40% per visit
Specialist:
In-Network: $45 per visit
Out-of-Network: 40% per visit
Preventive care
In-Network: $0 copay
Out-of-Network: $0 or 40%
View More
Benefits Services
Hearing exam In-Network: $45
Out-of-Network: 40%
Fitting/evaluation In-Network: $0 copay
Out-of-Network: $0 copay
There may be limits on how much the plan will provide.
Hearing aids In-Network: $699-999
Out-of-Network: $699-999
There may be limits on how much the plan will provide.
Optional Supplemental Benefits
Package #1 Comprehensive dental services, Preventive dental services
Monthly Premium $27.40
Deductible N/A
Drug Plan Information
Monthly Premium $0.00
Deductible $365
Formulary Website View formulary website
Return to previous page
https://www.medicare.gov/find-a-plan/results/planresults/plan-details.aspx?cntrctid=H5216&plnid=141&sgmntid=0#plan_benefits 2/2