
Page 39 - Cover Letter and Evaluation for Chris Parlin
P. 39
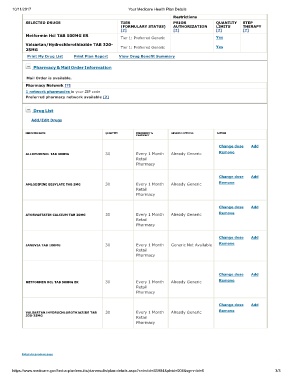
10/11/2017 Your Medicare Health Plan Details
Restrictions
SELECTED DRUGS TIER PRIOR QUANTITY STEP
(FORMULARY STATUS) AUTHORIZATION LIMITS THERAPY
[?] [?] [?] [?]
Metformin Hcl TAB 500MG ER
Tier 1: Preferred Generic Yes
Valsartan/Hydrochlorothiazide TAB 320- Yes
25MG Tier 1: Preferred Generic
Print My Drug List Print Plan Report View Drug Benefit Summary
Pharmacy & Mail Order Information
Mail Order is available.
Pharmacy Network [?]
1 network pharmacies in your ZIP code
Preferred pharmacy network available [?]
Drug List
Add/Edit Drugs
MEDICINE NAME QUANTITY FREQUENCY & GENERIC OPTIONS ACTION
PHARMACY
Change dose Add
ALLOPURINOL TAB 300MG 30 Every 1 Month Already Generic Remove
Retail
Pharmacy
Change dose Add
AMLODIPINE BESYLATE TAB 5MG 30 Every 1 Month Already Generic Remove
Retail
Pharmacy
Change dose Add
ATORVASTATIN CALCIUM TAB 20MG 30 Every 1 Month Already Generic Remove
Retail
Pharmacy
Change dose Add
JANUVIA TAB 100MG 30 Every 1 Month Generic Not Available Remove
Retail
Pharmacy
Change dose Add
METFORMIN HCL TAB 500MG ER 30 Every 1 Month Already Generic Remove
Retail
Pharmacy
Change dose Add
VALSARTAN/HYDROCHLOROTHIAZIDE TAB 30 Every 1 Month Already Generic Remove
320-25MG Retail
Pharmacy
Return to previous page
https://www.medicare.gov/find-a-plan/results/planresults/plan-details.aspx?cntrctid=S5884&plnid=004&sgmntid=0 3/3