
Page 66 - APPENDICES for Stephen Spero
P. 66
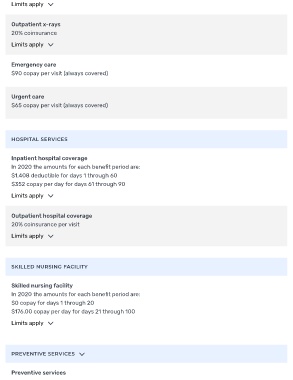
Limits apply
Outpatient x-rays
20% coinsurance
Limits apply
Emergency care
$90 copay per visit (always covered)
Urgent care
$65 copay per visit (always covered)
HOSPITAL SERVICES
Inpatient hospital coverage
In 2020 the amounts for each bene t period are:
$1,408 deductible for days 1 through 60
$352 copay per day for days 61 through 90
Limits apply
Outpatient hospital coverage
20% coinsurance per visit
Limits apply
SKILLED NURSING FACILITY
Skilled nursing facility
In 2020 the amounts for each bene t period are:
$0 copay for days 1 through 20
$176.00 copay per day for days 21 through 100
Limits apply
PREVENTIVE SERVICES
Preventive services