
Page 93 - APPENDICES for Stephen Spero
P. 93
Initial coveragenitial coverage G
I
Gap coverageap coverage
Catastrophic coverage phaseatastrophic coverage phase
T C
Tiersiers
phasehase phasehase
p
p
Preferred Generic $1.00 copay
Generic $2.00 copay
Generic drugs:
Generic drugs:
Preferred Brand $30.00 copay $3.60 copay or 5% (whichever costs
25%
more)
Non-Preferred
33% Brand-name
Drug Brand-name drugs:
drugs:
$8.95 copay or 5% (whichever costs
Specialty Tier 25% 25%
more)
Select Care
$0.00 copay
Drugs
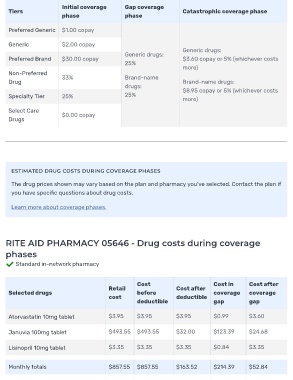
ESTIMATED DRUG COSTS DURING COVERAGE PHASES
The drug prices shown may vary based on the plan and pharmacy you've selected. Contact the plan if
you have speci c questions about drug costs.
Learn more about coverage phases.
RITE AID PHARMACY 05646 - Drug costs during coverage
phases
Standard in-network pharmacy
Cost Cost in Cost after
Retail Cost after
Selected drugs before coverage coverage
cost deductible
deductible gap gap
Atorvastatin 10mg tablet $3.95 $3.95 $3.95 $0.99 $3.60
Januvia 100mg tablet $493.55 $493.55 $32.00 $123.39 $24.68
Lisinopril 10mg tablet $3.35 $3.35 $3.35 $0.84 $3.35
Monthly totals $857.55 $857.55 $163.52 $214.39 $52.84