
Page 94 - Appendices to Donald Pender's Evaluation
P. 94
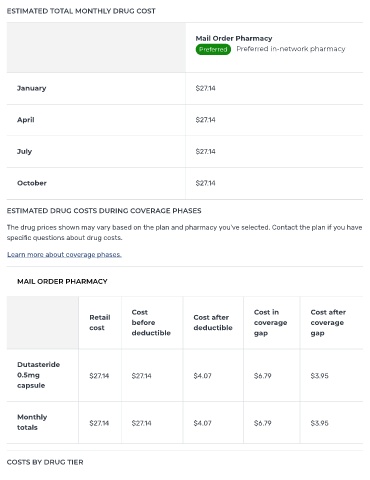
ESTIMATED TOTAL MONTHLY DRUG COST
Mail Order Pharmacy
Preferred Preferred in-network pharmacy
January $27.14
April $27.14
July $27.14
October $27.14
ESTIMATED DRUG COSTS DURING COVERAGE PHASES
The drug prices shown may vary based on the plan and pharmacy you've selected. Contact the plan if you have
speci c questions about drug costs.
Learn more about coverage phases.
MAIL ORDER PHARMACY
Cost Cost in Cost after
Retail Cost after
before coverage coverage
cost deductible
deductible gap gap
Dutasteride
0.5mg $27.14 $27.14 $4.07 $6.79 $3.95
capsule
Monthly
totals $27.14 $27.14 $4.07 $6.79 $3.95
COSTS BY DRUG TIER