
Page 116 - Cover Letter and Evaluation for John
P. 116
10/9/2018 Your Medicare Health Plan Details
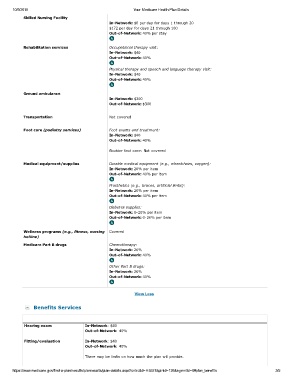
Skilled Nursing Facility
In-Network: $0 per day for days 1 through 20
$172 per day for days 21 through 100
Out-of-Network: 40% per stay
Rehabilitation services Occupational therapy visit:
In-Network: $40
Out-of-Network: 40%
Physical therapy and speech and language therapy visit:
In-Network: $40
Out-of-Network: 40%
Ground ambulance
In-Network: $300
Out-of-Network: $300
Transportation Not covered
Foot care (podiatry services) Foot exams and treatment:
In-Network: $40
Out-of-Network: 40%
Routine foot care: Not covered
Medical equipment/supplies Durable medical equipment (e.g., wheelchairs, oxygen):
In-Network: 20% per item
Out-of-Network: 40% per item
Prosthetics (e.g., braces, artificial limbs):
In-Network: 20% per item
Out-of-Network: 40% per item
Diabetes supplies:
In-Network: 0-20% per item
Out-of-Network: 0-20% per item
Wellness programs (e.g., fitness, nursing Covered
hotline)
Medicare Part B drugs Chemotherapy:
In-Network: 20%
Out-of-Network: 40%
Other Part B drugs:
In-Network: 20%
Out-of-Network: 40%
View Less
Benefits Services
Hearing exam In-Network: $40
Out-of-Network: 40%
Fitting/evaluation In-Network: $40
Out-of-Network: 40%
There may be limits on how much the plan will provide.
https://www.medicare.gov/find-a-plan/results/planresults/plan-details.aspx?cntrctid=H5521&plnid=126&sgmntid=0#plan_benefits 3/5