
Page 68 - Evaluation for 2018
P. 68
1/3/2018 Your Medicare Health Plan Details
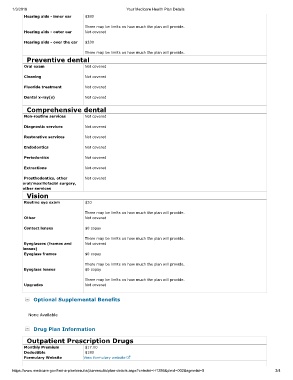
Hearing aids - inner ear $380
There may be limits on how much the plan will provide.
Hearing aids - outer ear Not covered
Hearing aids - over the ear $330
There may be limits on how much the plan will provide.
Preventive dental
Oral exam Not covered
Cleaning Not covered
Fluoride treatment Not covered
Dental x-ray(s) Not covered
Comprehensive dental
Non-routine services Not covered
Diagnostic services Not covered
Restorative services Not covered
Endodontics Not covered
Periodontics Not covered
Extractions Not covered
Prosthodontics, other Not covered
oral/maxillofacial surgery,
other services
Vision
Routine eye exam $20
There may be limits on how much the plan will provide.
Other Not covered
Contact lenses $0 copay
There may be limits on how much the plan will provide.
Eyeglasses (frames and Not covered
lenses)
Eyeglass frames $0 copay
There may be limits on how much the plan will provide.
Eyeglass lenses $0 copay
There may be limits on how much the plan will provide.
Upgrades Not covered
Optional Supplemental Benefits
None Available
Drug Plan Information
Outpatient Prescription Drugs
Monthly Premium $17.00
Deductible $180
Formulary Website View formulary website
https://www.medicare.gov/find-a-plan/results/planresults/plan-details.aspx?cntrctid=H1286&plnid=002&sgmntid=0 3/4