
Page 83 - Evaluation for 2018
P. 83
12/23/2017 Your Medicare Health Plan Details
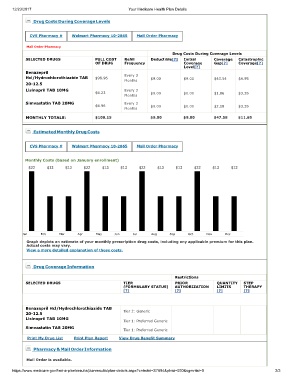
Drug Costs During Coverage Levels
CVS Pharmacy # Walmart Pharmacy 10-2865 Mail Order Pharmacy
Mail Order Pharmacy
Drug Costs During Coverage Levels
SELECTED DRUGS FULL COST Refill Deductible[?] Initial Coverage Catastrophic
OF DRUG Frequency Coverage Gap[?] Coverage[?]
Level[?]
Benazepril
Hcl/Hydrochlorothiazide TAB $98.96 Every 3 $9.00 $9.00 $43.54 $4.95
Months
20-12.5
Lisinopril TAB 10MG Every 3
$4.23 $0.00 $0.00 $1.86 $3.35
Months
Simvastatin TAB 20MG Every 3
$4.96 $0.00 $0.00 $2.18 $3.35
Months
MONTHLY TOTALS: $108.15 $9.00 $9.00 $47.58 $11.65
Estimated Monthly Drug Costs
CVS Pharmacy # Walmart Pharmacy 10-2865 Mail Order Pharmacy
Monthly Costs (based on January enrollment)
$22 $13 $13 $22 $13 $13 $22 $13 $13 $22 $13 $13
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Graph depicts an estimate of your monthly prescription drug costs, including any applicable premium for this plan.
Actual costs may vary.
View a more detailed explanation of these costs.
Drug Coverage Information
Restrictions
SELECTED DRUGS TIER PRIOR QUANTITY STEP
(FORMULARY STATUS) AUTHORIZATION LIMITS THERAPY
[?] [?] [?] [?]
Benazepril Hcl/Hydrochlorothiazide TAB
20-12.5 Tier 2: Generic
Lisinopril TAB 10MG
Tier 1: Preferred Generic
Simvastatin TAB 20MG
Tier 1: Preferred Generic
Print My Drug List Print Plan Report View Drug Benefit Summary
Pharmacy & Mail Order Information
Mail Order is available.
https://www.medicare.gov/find-a-plan/results/planresults/plan-details.aspx?cntrctid=S7694&plnid=030&sgmntid=0 2/3