
Page 66 - Cover Letter and Evaluation for Mike Peaseley
P. 66
11/17/2017 Your Medicare Health Plan Comparison
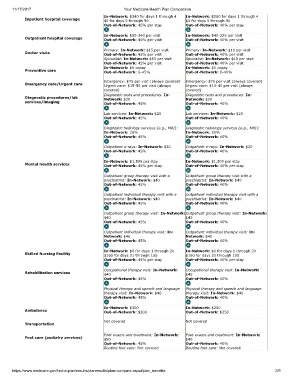
In-Network: $340 for days 1 through 4 In-Network: $250 for days 1 through 4
Inpatient hospital coverage $0 for days 5 through 90 $0 for days 5 through 90
Out-of-Network: 45% per stay Out-of-Network: 40% per stay
In-Network: $50-340 per visit In-Network: $40-225 per visit
Outpatient hospital coverage Out-of-Network: 45% per visit Out-of-Network: 40% per visit
Primary: In-Network: $15 per visit Primary: In-Network: $10 per visit
Doctor visits Out-of-Network: 45% per visit Out-of-Network: 40% per visit
Specialist: In-Network: $50 per visit Specialist: In-Network: $40 per visit
Out-of-Network: 45% per visit Out-of-Network: 40% per visit
In-Network: $0 copay In-Network: $0 copay
Preventive care Out-of-Network: 0-45% Out-of-Network: 0-40%
Emergency: $75 per visit (always covered) Emergency: $75 per visit (always covered)
Emergency care/Urgent care Urgent care: $15-50 per visit (always Urgent care: $10-40 per visit (always
covered) covered)
Diagnostic tests and procedures: In- Diagnostic tests and procedures: In-
Diagnostic procedures/lab Network: $20 Network: $20
services/imaging Out-of-Network: 45% Out-of-Network: 40%
Lab services: In-Network: $20 Lab services: In-Network: $20
Out-of-Network: 45% Out-of-Network: 40%
Diagnostic radiology services (e.g., MRI): Diagnostic radiology services (e.g., MRI):
In-Network: 20% In-Network: 20%
Out-of-Network: 45% Out-of-Network: 40%
Outpatient x-rays: In-Network: $20 Outpatient x-rays: In-Network: $20
Out-of-Network: 45% Out-of-Network: 40%
In-Network: $1,500 per stay In-Network: $1,500 per stay
Mental health services Out-of-Network: 45% per stay Out-of-Network: 40% per stay
Outpatient group therapy visit with a Outpatient group therapy visit with a
psychiatrist: In-Network: $40 psychiatrist: In-Network: $40
Out-of-Network: 45% Out-of-Network: 40%
Outpatient individual therapy visit with a Outpatient individual therapy visit with a
psychiatrist: In-Network: $40 psychiatrist: In-Network: $40
Out-of-Network: 45% Out-of-Network: 40%
Outpatient group therapy visit: In-Network: Outpatient group therapy visit: In-Network:
$40 $40
Out-of-Network: 45% Out-of-Network: 40%
Outpatient individual therapy visit: In- Outpatient individual therapy visit: In-
Network: $40 Network: $40
Out-of-Network: 45% Out-of-Network: 40%
In-Network: $0 for days 1 through 20 In-Network: $0 for days 1 through 20
Skilled Nursing Facility $160 for days 21 through 100 $160 for days 21 through 100
Out-of-Network: 45% per stay Out-of-Network: 40% per stay
Occupational therapy visit: In-Network: Occupational therapy visit: In-Network:
Rehabilitation services $40 $40
Out-of-Network: 45% Out-of-Network: 40%
Physical therapy and speech and language Physical therapy and speech and language
therapy visit: In-Network: $40 therapy visit: In-Network: $40
Out-of-Network: 45% Out-of-Network: 40%
In-Network: $300 In-Network: $250
Ambulance Out-of-Network: $300 Out-of-Network: $250
Not covered Not covered
Transportation
Foot exams and treatment: In-Network: Foot exams and treatment: In-Network:
Foot care (podiatry services) $50 $40
Out-of-Network: 45% Out-of-Network: 40%
Routine foot care: Not covered Routine foot care: Not covered
https://www.medicare.gov/find-a-plan/results/planresults/plan-compare.aspx#plan_benefits 2/9