
Page 81 - Cover Letter and Evaluation for Mike Peaseley
P. 81
11/17/2017 Your Medicare Health Plan Details
Drug Plan Information
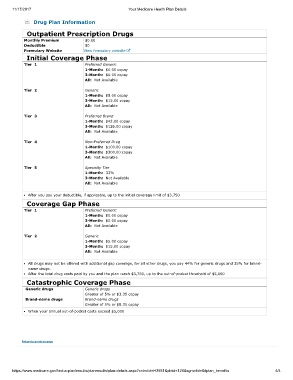
Outpatient Prescription Drugs
Monthly Premium $0.00
Deductible $0
Formulary Website View formulary website
Initial Coverage Phase
Tier 1 Preferred Generic
1-Month: $0.00 copay
3-Month: $0.00 copay
All: Not Available
Tier 2 Generic
1-Month: $5.00 copay
3-Month: $15.00 copay
All: Not Available
Tier 3 Preferred Brand
1-Month: $42.00 copay
3-Month: $126.00 copay
All: Not Available
Tier 4 Non-Preferred Drug
1-Month: $100.00 copay
3-Month: $300.00 copay
All: Not Available
Tier 5 Specialty Tier
1-Month: 33%
3-Month: Not Available
All: Not Available
After you pay your deductible, if applicable, up to the initial coverage limit of $3,750
Coverage Gap Phase
Tier 1 Preferred Generic
1-Month: $0.00 copay
3-Month: $0.00 copay
All: Not Available
Tier 2 Generic
1-Month: $5.00 copay
3-Month: $15.00 copay
All: Not Available
All drugs may not be offered with additional gap coverage, for all other drugs, you pay 44% for generic drugs and 35% for brand-
name drugs.
After the total drug costs paid by you and the plan reach $3,750, up to the out-of-pocket threshold of $5,000
Catastrophic Coverage Phase
Generic drugs Generic drugs
Greater of 5% or $3.35 copay
Brand-name drugs Brand-name drugs
Greater of 5% or $8.35 copay
When your annual out-of-pocket costs exceed $5,000
Return to previous page
https://www.medicare.gov/find-a-plan/results/planresults/plan-details.aspx?cntrctid=H3931&plnid=126&sgmntid=0#plan_benefits 4/4