
Page 159 - Cover Letter and Evaluation for Gary Janke
P. 159
10/8/2018 Your Medicare Health Plan Details
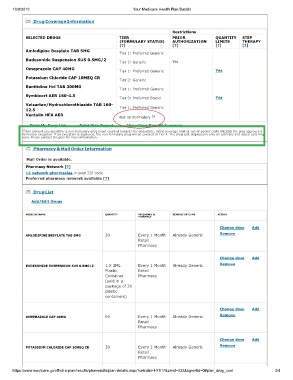
Drug Coverage Information
Restrictions
SELECTED DRUGS TIER PRIOR QUANTITY STEP
(FORMULARY STATUS) AUTHORIZATION LIMITS THERAPY
[?] [?] [?] [?]
Amlodipine Besylate TAB 5MG
Tier 1: Preferred Generic
Budesonide Suspension SUS 0.5MG/2
Tier 2: Generic Yes
Omeprazole CAP 40MG
Tier 1: Preferred Generic Yes
Potassium Chloride CAP 10MEQ CR
Tier 2: Generic
Ranitidine Hcl TAB 300MG
Tier 1: Preferred Generic
Symbicort AER 160-4.5
Tier 3: Preferred Brand Yes
Valsartan/Hydrochlorothiazide TAB 160-
12.5 Tier 1: Preferred Generic
Ventolin HFA AER 15
Not on Formulary
Print My Drug List Print Plan Report View Drug Benefit Summary
15 Any amount you spend for a non-formulary drug is not counted towards the deductible, initial coverage limit or out-of-pocket costs UNLESS the plan approves a
formulary exception. If an exception is approved, the non-formulary drug will be covered at Tier 4. The drug cost displayed is only an estimate and actual cost may
vary. Please contact the plan for more information.
Pharmacy & Mail Order Information
Mail Order is available.
Pharmacy Network [?]
13 network pharmacies in your ZIP code
Preferred pharmacy network available [?]
Drug List
Add/Edit Drugs
MEDICINE NAME QUANTITY FREQUENCY & GENERIC OPTIONS ACTION
PHARMACY
Change dose Add
AMLODIPINE BESYLATE TAB 5MG 30 Every 1 Month Already Generic Remove
Retail
Pharmacy
Change dose Add
BUDESONIDE SUSPENSION SUS 0.5MG/2 1 X 2ML Every 1 Month Already Generic Remove
Plastic Retail
Container Pharmacy
(sold in a
package of 30
plastic
containers)
Change dose Add
OMEPRAZOLE CAP 40MG 60 Every 1 Month Already Generic Remove
Retail
Pharmacy
Change dose Add
POTASSIUM CHLORIDE CAP 10MEQ CR 30 Every 1 Month Already Generic Remove
Retail
Pharmacy
https://www.medicare.gov/find-a-plan/results/planresults/plan-details.aspx?cntrctid=H7917&plnid=032&sgmntid=0#plan_drug_cost 3/4