
Page 89 - Appendices to Jane Miller's evaluation
P. 89
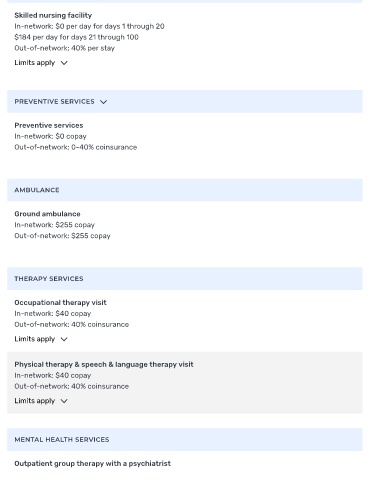
Skilled nursing facility
In-network: $0 per day for days 1 through 20
$184 per day for days 21 through 100
Out-of-network: 40% per stay
Limits apply
PREVENTIVE SERVICES
Preventive services
In-network: $0 copay
Out-of-network: 0-40% coinsurance
AMBULANCE
Ground ambulance
In-network: $255 copay
Out-of-network: $255 copay
THERAPY SERVICES
Occupational therapy visit
In-network: $40 copay
Out-of-network: 40% coinsurance
Limits apply
Physical therapy & speech & language therapy visit
In-network: $40 copay
Out-of-network: 40% coinsurance
Limits apply
MENTAL HEALTH SERVICES
Outpatient group therapy with a psychiatrist