Page 5 - Yaskawa 2022 Open Enrollment Guide
P. 5
2022 Benefits Guide
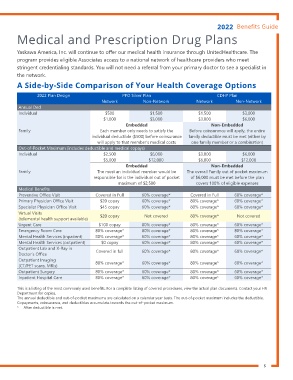
Medical and Prescription Drug Plans
Yaskawa America, Inc. will continue to ofer our medical health insurance through UnitedHealthcare. The
program provides eligible Associates access to a national network of healthcare providers who meet
stringent credentialing standards. You will not need a referral from your primary doctor to see a specialist in
the network.
A Side-by-Side Comparison of Your Health Coverage Options
2022 Plan Design PPO Silver Plan CDHP Plan
Network Non-Network Network Non-Network
Annual Ded
Individual $500 $1,500 $1,500 $3,000
$1,000 $3,000 $3,000 $6,000
Embedded Non-Embedded
Family Each member only needs to satisfy the Before coinsurance will apply, the entire
individual deductible ($500) before coinsurance family deductible must be met (either by
will apply to that member’s medical costs one family member or a combination)
Out-of-Pocket Maximum (includes deductible and medical copays)
Individual $2,500 $6,000 $3,000 $6,000
$5,000 $12,000 $6,000 $12,000
Embedded Non-Embedded
Family The most an individual member would be The overall Family out of pocket maximum
responsible for is the individual out of pocket of $6,000 must be met before the plan
maximum of $2,500 covers 100% of eligible expenses
Medical Beneits
Preventive Oice Visit Covered in Full 60% coverage* Covered in Full 60% coverage*
Primary Physician Oice Visit $20 copay 60% coverage* 80% coverage* 60% coverage*
Specialist Physician Oice Visit $45 copay 60% coverage* 80% coverage* 60% coverage*
Virtual Visits $20 copay Not covered 80% coverage* Not covered
(telemental health support available)
Urgent Care $100 copay 80% coverage* 80% coverage* 60% coverage*
Emergency Room Care 80% coverage* 80% coverage* 80% coverage* 80% coverage*
Mental Health Services (inpatient) 80% coverage* 60% coverage* 80% coverage* 60% coverage*
Mental Health Services (outpatient) $0 copay 60% coverage* 80% coverage* 60% coverage*
Outpatient Lab and X-Ray in Covered in full 60% coverage* 80% coverage* 60% coverage*
Doctor’s Oice
Outpatient Imaging 80% coverage* 60% coverage* 80% coverage* 60% coverage*
(CT/PET scans, MRIs)
Outpatient Surgery 80% coverage* 60% coverage* 80% coverage* 60% coverage*
Inpatient Hospital Care 80% coverage* 60% coverage* 80% coverage* 60% coverage*
This is a listing of the most commonly used beneits. For a complete listing of covered procedures, view the actual plan documents. Contact your HR
Department for copies.
The annual deductible and out-of-pocket maximums are calculated on a calendar year basis. The out-of-pocket maximum includes the deductible.
Copayments, coinsurance, and deductibles accumulate towards the out-of-pocket maximum.
* After deductible is met.
5
Medical and Prescription Drug Plans
Yaskawa America, Inc. will continue to ofer our medical health insurance through UnitedHealthcare. The
program provides eligible Associates access to a national network of healthcare providers who meet
stringent credentialing standards. You will not need a referral from your primary doctor to see a specialist in
the network.
A Side-by-Side Comparison of Your Health Coverage Options
2022 Plan Design PPO Silver Plan CDHP Plan
Network Non-Network Network Non-Network
Annual Ded
Individual $500 $1,500 $1,500 $3,000
$1,000 $3,000 $3,000 $6,000
Embedded Non-Embedded
Family Each member only needs to satisfy the Before coinsurance will apply, the entire
individual deductible ($500) before coinsurance family deductible must be met (either by
will apply to that member’s medical costs one family member or a combination)
Out-of-Pocket Maximum (includes deductible and medical copays)
Individual $2,500 $6,000 $3,000 $6,000
$5,000 $12,000 $6,000 $12,000
Embedded Non-Embedded
Family The most an individual member would be The overall Family out of pocket maximum
responsible for is the individual out of pocket of $6,000 must be met before the plan
maximum of $2,500 covers 100% of eligible expenses
Medical Beneits
Preventive Oice Visit Covered in Full 60% coverage* Covered in Full 60% coverage*
Primary Physician Oice Visit $20 copay 60% coverage* 80% coverage* 60% coverage*
Specialist Physician Oice Visit $45 copay 60% coverage* 80% coverage* 60% coverage*
Virtual Visits $20 copay Not covered 80% coverage* Not covered
(telemental health support available)
Urgent Care $100 copay 80% coverage* 80% coverage* 60% coverage*
Emergency Room Care 80% coverage* 80% coverage* 80% coverage* 80% coverage*
Mental Health Services (inpatient) 80% coverage* 60% coverage* 80% coverage* 60% coverage*
Mental Health Services (outpatient) $0 copay 60% coverage* 80% coverage* 60% coverage*
Outpatient Lab and X-Ray in Covered in full 60% coverage* 80% coverage* 60% coverage*
Doctor’s Oice
Outpatient Imaging 80% coverage* 60% coverage* 80% coverage* 60% coverage*
(CT/PET scans, MRIs)
Outpatient Surgery 80% coverage* 60% coverage* 80% coverage* 60% coverage*
Inpatient Hospital Care 80% coverage* 60% coverage* 80% coverage* 60% coverage*
This is a listing of the most commonly used beneits. For a complete listing of covered procedures, view the actual plan documents. Contact your HR
Department for copies.
The annual deductible and out-of-pocket maximums are calculated on a calendar year basis. The out-of-pocket maximum includes the deductible.
Copayments, coinsurance, and deductibles accumulate towards the out-of-pocket maximum.
* After deductible is met.
5