
Page 5 - 2022 Benefit Guide FNA Combustion
P. 5
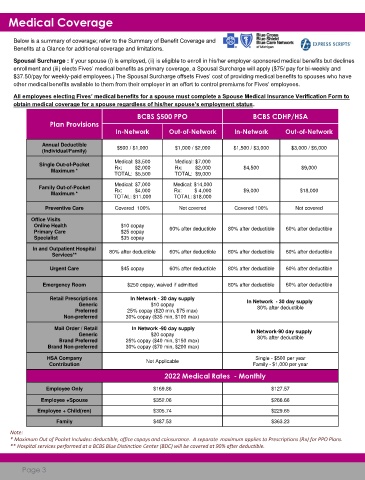
Medical Coverage
Below is a summary of coverage; refer to the Summary of Benefit Coverage and
Benefits at a Glance for additional coverage and limitations.
Spousal Surcharge : If your spouse (i) is employed, (ii) is eligible to enroll in his/her employer-sponsored medical benefits but declines
enrollment and (iii) elects Fives’ medical benefits as primary coverage, a Spousal Surcharge will apply ($75/ pay for bi-weekly and
$37.50/pay for weekly-paid employees.) The Spousal Surcharge offsets Fives’ cost of providing medical benefits to spouses who have
other medical benefits available to them from their employer in an effort to control premiums for Fives’ employees.
All employees electing Fives’ medical benefits for a spouse must complete a Spouse Medical Insurance Verification Form to
obtain medical coverage for a spouse regardless of his/her spouse’s employment status.
BCBS $500 PPO BCBS CDHP/HSA
Plan Provisions
In-Network Out-of-Network In-Network Out-of-Network
Annual Deductible $500 / $1,000 $1,000 / $2,000 $1,500 / $3,000 $3,000 / $6,000
(Individual/Family)
Medical: $3,500 Medical: $7,000
Single Out-of-Pocket
Maximum * Rx: $2,000 Rx: $2,000 $4,500 $9,000
TOTAL: $5,500 TOTAL: $9,000
Medical: $7,000 Medical: $14,000
Family Out-of-Pocket
Maximum * Rx: $4,000 Rx: $ 4,000 $9,000 $18,000
TOTAL: $11,000 TOTAL: $18,000
Preventive Care Covered 100% Not covered Covered 100% Not covered
Office Visits
Online Health $10 copay
Primary Care $25 copay 60% after deductible 80% after deductible 60% after deductible
Specialist $35 copay
In and Outpatient Hospital 80% after deductible 60% after deductible 80% after deductible 60% after deductible
Services**
Urgent Care $45 copay 60% after deductible 80% after deductible 60% after deductible
Emergency Room $250 copay, waived if admitted 80% after deductible 60% after deductible
Retail Prescriptions In Network - 30 day supply In Network - 30 day supply
Generic $10 copay
Preferred 25% copay ($20 min, $75 max) 80% after deductible
Non-preferred 30% copay ($35 min, $100 max)
Mail Order / Retail In Network -90 day supply In Network-90 day supply
Generic $20 copay
Brand Preferred 25% copay ($40 min, $150 max) 80% after deductible
Brand Non-preferred 30% copay ($70 min, $200 max)
HSA Company Not Applicable Single - $500 per year
Contribution Family - $1,000 per year
2022 Medical Rates - Monthly
(bi-weekly)
Employee Only $169.86 $127.57
Employee +Spouse $352.06 $266.66
Employee + Child(ren) $305.74 $229.65
Family $487.53 $363.23
Note:
* Maximum Out of Pocket Includes: deductible, office copays and coinsurance. A separate maximum applies to Prescriptions (Rx) for PPO Plans.
** Hospital services performed at a BCBS Blue Distinction Center (BDC) will be covered at 90% after deductible.
Page 3