
Page 7 - Impact Floors 2022 Benefit Guide
P. 7
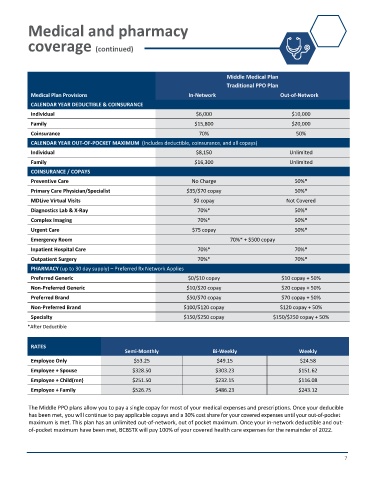
Medical and pharmacy
coverage (continued)
Middle Medical Plan
Traditional PPO Plan
Medical Plan Provisions In-Network Out-of-Network
CALENDAR YEAR DEDUCTIBLE & COINSURANCE
Individual $6,000 $10,000
Family $15,800 $20,000
Coinsurance 70% 50%
CALENDAR YEAR OUT-OF-POCKET MAXIMUM (Includes deductible, coinsurance, and all copays)
Individual $8,150 Unlimited
Family $16,300 Unlimited
COINSURANCE / COPAYS
Preventive Care No Charge 50%*
Primary Care Physician/Specialist $35/$70 copay 50%*
MDLive Virtual Visits $0 copay Not Covered
Diagnostics Lab & X-Ray 70%* 50%*
Complex Imaging 70%* 50%*
Urgent Care $75 copay 50%*
Emergency Room 70%* + $500 copay
Inpatient Hospital Care 70%* 70%*
Outpatient Surgery 70%* 70%*
PHARMACY (up to 30 day supply) – Preferred Rx Network Applies
Preferred Generic $0/$10 copay $10 copay + 50%
Non-Preferred Generic $10/$20 copay $20 copay + 50%
Preferred Brand $50/$70 copay $70 copay + 50%
Non-Preferred Brand $100/$120 copay $120 copay + 50%
Specialty $150/$250 copay $150/$250 copay + 50%
*After Deductible
RATES
Semi-Monthly Bi-Weekly Weekly
Employee Only $53.25 $49.15 $24.58
Employee + Spouse $328.50 $303.23 $151.62
Employee + Child(ren) $251.50 $232.15 $116.08
Employee + Family $526.75 $486.23 $243.12
The Middle PPO plans allow you to pay a single copay for most of your medical expenses and prescriptions. Once your deducible
has been met, you will continue to pay applicable copays and a 30% cost share for your covered expenses until your out-of-pocket
maximum is met. This plan has an unlimited out-of-network, out of pocket maximum. Once your in-network deductible and out-
of-pocket maximum have been met, BCBSTX will pay 100% of your covered health care expenses for the remainder of 2022.
7