
Page 8 - Commissioners Office
P. 8
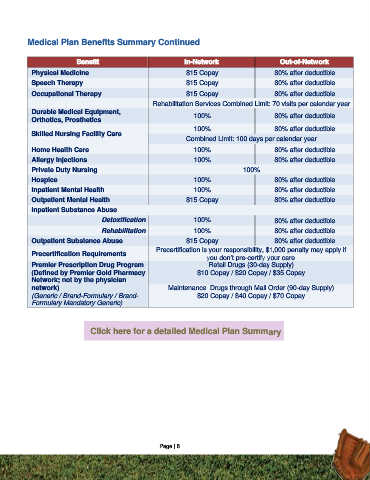
Medical Plan Benefits Summary Continued
Benefit In-Network Out-of-Network
Physical Medicine $15 Copay 80% after deductible
Speech Therapy $15 Copay 80% after deductible
Occupational Therapy $15 Copay 80% after deductible
Rehabilitation Services Combined Limit: 70 visits per calendar year
Durable Medical Equipment, 100% 80% after deductible
Orthotics, Prosthetics
100% 80% after deductible
Skilled Nursing Facility Care
Combined Limit: 100 days per calendar year
Home Health Care 100% 80% after deductible
Allergy Injections 100% 80% after deductible
Private Duty Nursing 100%
Hospice 100% 80% after deductible
Inpatient Mental Health 100% 80% after deductible
Outpatient Mental Health $15 Copay 80% after deductible
Inpatient Substance Abuse
Detoxification 100% 80% after deductible
Rehabilitation 100% 80% after deductible
Outpatient Substance Abuse $15 Copay 80% after deductible
Precertification is your responsibility, $1,000 penalty may apply if
Precertification Requirements
you don’t pre-certify your care
Premier Prescription Drug Program Retail Drugs (30-day Supply)
(Defined by Premier Gold Pharmacy $10 Copay / $20 Copay / $35 Copay
Network; not by the physician
network) Maintenance Drugs through Mail Order (90-day Supply)
(Generic / Brand-Formulary / Brand- $20 Copay / $40 Copay / $70 Copay
Formulary Mandatory Generic)
Click here for a detailed Medical Plan Summary
Page | 8