
Page 13 - Washington Nationals 2023 Benefits Guide -10.26.22_Neat
P. 13
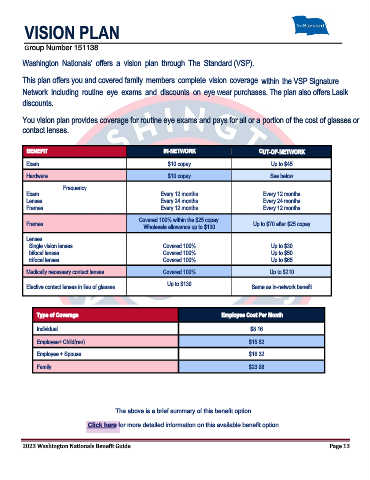
VISION PLAN
Group Number 151138
Washington Nationals' offers a vision plan through The Standard (VSP).
This plan offers you and covered family members complete vision coverage within the VSP Signature
Network including routine eye exams and discounts on eye wear purchases. The plan also offers Lasik
discounts.
You vision plan provides coverage for routine eye exams and pays for all or a portion of the cost of glasses or
contact lenses.
BENEFIT IN-NETWORK OUT-OF-NETWORK
Exam $10 copay Up to $45
Hardware $10 copay See below
Frequency
Exam Every 12 months Every 12 months
Lenses Every 24 months Every 24 months
Frames Every 12 months Every 12 months
Covered 100% within the $25 copay.
Frames Up to $70 after $25 copay
Wholesale allowance up to $130
Lenses
Single vision lenses Covered 100% Up to $30
bifocal lenses Covered 100% Up to $50
trifocal lenses Covered 100% Up to $65
Medically necessary contact lenses Covered 100% Up to $210
Up to $130
Elective contact lenses in lieu of glasses Same as in-network benefit
Type of Coverage Employee Cost Per Month
Individual $8.16
Employee+ Child(ren) $15.52
Employee + Spouse $16.32
Family $23.68
The above is a brief summary of this benefit option.
Click here for more detailed information on this available benefit option.
2023 Washington Nationals Benefit Guide Page 13