
Page 3 - 2021 01 Benefits Guide Murata FINAL
P. 3
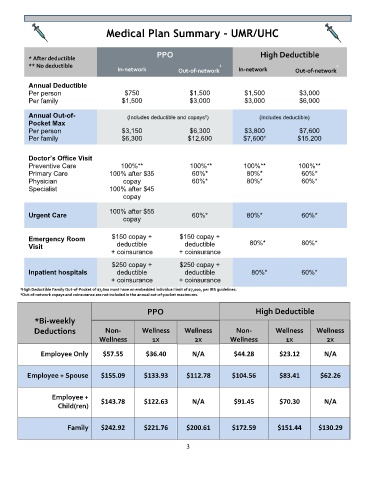
Medical Plan Summary – UMR/UHC
* After deductible PPO High Deductible
** No deductible 1 1
In-network Out-of-network In-network Out-of-network
Annual Deductible
Per person $750 $1,500 $1,500 $3,000
Per family $1,500 $3,000 $3,000 $6,000
Annual Out-of- (Includes deductible and copays²) (Includes deductible)
Pocket Max
Per person $3,150 $6,300 $3,800 $7,600
Per family $6,300 $12,600 $7,600¹ $15,200
Doctor’s Office Visit
Preventive Care 100%** 100%** 100%** 100%**
Primary Care 100% after $35 60%* 80%* 60%*
Physician copay 60%* 80%* 60%*
Specialist 100% after $45
copay
Urgent Care 100% after $55 60%* 80%* 60%*
copay
Emergency Room $150 copay + $150 copay +
Visit deductible deductible 80%* 80%*
+ coinsurance + coinsurance
$250 copay + $250 copay +
Inpatient hospitals deductible deductible 80%* 60%*
+ coinsurance + coinsurance
¹High Deductible Family Out-of-Pocket of $7,600 must have an embedded individual limit of $7,000, per IRS guidelines.
²Out-of-network copays and coinsurance are not included in the annual out-of-pocket maximums.
PPO High Deductible
*Bi-weekly
Deductions Non- Wellness Wellness Non- Wellness Wellness
Wellness 1X 2X Wellness 1X 2X
Employee Only $57.55 $36.40 N/A $44.28 $23.12 N/A
Employee + Spouse $155.09 $133.93 $112.78 $104.56 $83.41 $62.26
Employee +
$143.78 $122.63 N/A $91.45 $70.30 N/A
Child(ren)
Family $242.92 $221.76 $200.61 $172.59 $151.44 $130.29
3