
Page 7 - 2021 01 Benefits Guide Murata FINAL
P. 7
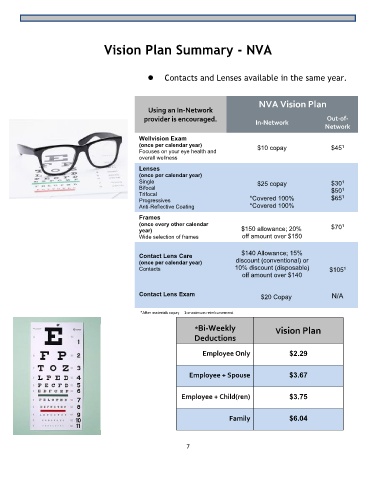
Vision Plan Summary - NVA
⚫ Contacts and Lenses available in the same year.
NVA Vision Plan
Using an In-Network
provider is encouraged. Out-of-
In-Network
Network
Wellvision Exam
(once per calendar year) $10 copay $45
1
Focuses on your eye health and
overall wellness
Lenses
(once per calendar year)
Single $25 copay $30
1
Bifocal $50
1
Trifocal 1
Progressives *Covered 100% $65
Anti-Reflective Coating *Covered 100%
Frames
(once every other calendar $70
1
year) $150 allowance; 20%
Wide selection of frames off amount over $150
Contact Lens Care $140 Allowance; 15%
(once per calendar year) discount (conventional) or
1
Contacts 10% discount (disposable) $105
off amount over $140
Contact Lens Exam $20 Copay N/A
*After materials copay 1=maximum reimbursement
*Bi-Weekly
Vision Plan
Deductions
Employee Only $2.29
Employee + Spouse $3.67
Employee + Child(ren) $3.75
Family $6.04
7