
Page 6 - Mitsubishi-2022-Benefit Guide-MCPP-V9(JO)-LRI_Neat
P. 6
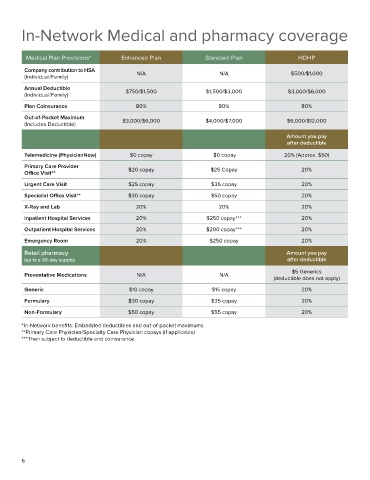
In-Network Medical and pharmacy coverage
Medical Plan Provisions* Enhanced Plan Standard Plan HDHP
Company contribution to HSA N/A N/A $500/$1,000
(Individual/Family)
Annual Deductible
(Individual/Family) $750/$1,500 $1,500/$3,000 $3,000/$6,000
Plan Coinsurance 80% 80% 80%
Out-of-Pocket Maximum $3,000/$6,000 $4,000/$7,000 $6,000/$12,000
(Includes Deductible)
Amount you pay
after deductible
Telemedicine (PhysicianNow) $0 copay $0 copay 20% (Approx. $50)
Primary Care Provider
Office Visit** $20 copay $25 Copay 20%
Urgent Care Visit $25 copay $35 copay 20%
Specialist Office Visit** $30 copay $50 copay 20%
X-Ray and Lab 20% 20% 20%
Inpatient Hospital Services 20% $250 copay*** 20%
Outpatient Hospital Services 20% $200 copay*** 20%
Emergency Room 20% $250 copay 20%
Retail pharmacy Amount you pay
(up to a 30-day supply) after deductible
Preventative Medications N/A N/A $5 Generics
(deductible does not apply)
Generic $10 copay $15 copay 20%
Formulary $30 copay $35 copay 20%
Non-Formulary $50 copay $55 copay 20%
*In-Network benefits. Embedded deductibles and out-of-pocket maximums.
**Primary Care Physician/Specialty Care Physician copays (if applicable)
***Then subject to deductible and coinsurance
6