
Page 7 - 2023 Down East Wood Ducks - Benefits Guide.docx_Neat
P. 7
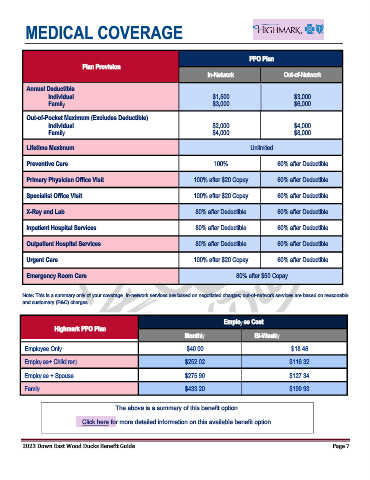
MEDICAL COVERAGE
PPO Plan
Plan Provision
In-Network Out-of-Network
Annual Deductible
Individual $1,500 $3,000
Family $3,000 $6,000
Out-of-Pocket Maximum (Excludes Deductible)
Individual $2,000 $4,000
Family $4,000 $8,000
Lifetime Maximum Unlimited
Preventive Care 100% 60% after Deductible
Primary Physician Office Visit 100% after $20 Copay 60% after Deductible
Specialist Office Visit 100% after $20 Copay 60% after Deductible
X-Ray and Lab 80% after Deductible 60% after Deductible
Inpatient Hospital Services 80% after Deductible 60% after Deductible
Outpatient Hospital Services 80% after Deductible 60% after Deductible
Urgent Care 100% after $20 Copay 60% after Deductible
Emergency Room Care 80% after $50 Copay
Note: This is a summary only of your coverage. In-network services are based on negotiated charges; out-of-network services are based on reasonable
and customary (R&C) charges.
Employee Cost
Highmark PPO Plan
Monthly Bi-Weekly
Employee Only $40.00 $18.46
Employee+ Child(ren) $252.02 $116.32
Employee + Spouse $275.90 $127.34
Family $433.20 $199.93
The above is a summary of this benefit option.
Click here for more detailed information on this available benefit option.
2023 Down East Wood Ducks Benefit Guide Page 7