
Page 6 - AFL 2022 Grandfathered Guide with Legal Notices
P. 6
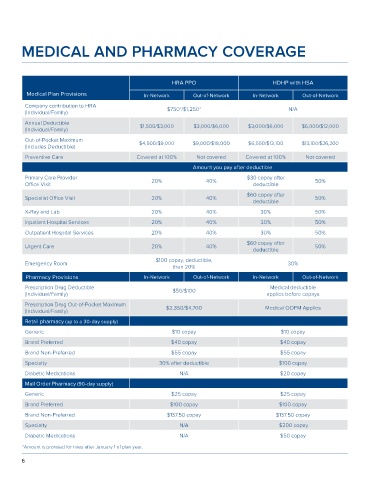
MEDICAL AND PHARMACY COVERAGE
HRA PPO HDHP with HSA
Medical Plan Provisions In-Network Out-of-Network In-Network Out-of-Network
Company contribution to HRA 2 2
(Individual/Family) $750 /$1,250 N/A
Annual Deductible $1,500/$3,000 $3,000/$6,000 $3,000/$6,000 $6,000/$12,000
(Individual/Family)
Out-of-Pocket Maximum $4,500/$9,000 $9,000/$18,000 $6,550/$13,100 $13,100/$26,200
(Includes Deductible)
Preventive Care Covered at 100% Not covered Covered at 100% Not covered
Amount you pay after deductible
Primary Care Provider 20% 40% $30 copay after 50%
Office Visit deductible
$60 copay after
Specialist Office Visit 20% 40% 50%
deductible
X-Ray and Lab 20% 40% 30% 50%
Inpatient Hospital Services 20% 40% 30% 50%
Outpatient Hospital Services 20% 40% 30% 50%
$60 copay after
Urgent Care 20% 40% 50%
deductible
$100 copay, deductible,
Emergency Room 30%
then 20%
Pharmacy Provisions In-Network Out-of-Network In-Network Out-of-Network
Prescription Drug Deductible $50/$100 Medical deductible
(Individual/Family) applies before copays
Prescription Drug Out-of-Pocket Maximum
(Individual/Family) $2,350/$4,700 Medical OOPM Applies
Retail pharmacy (up to a 30-day supply)
Generic $10 copay $10 copay
Brand Preferred $40 copay $40 copay
Brand Non-Preferred $55 copay $55 copay
Specialty 30% after deductible $100 copay
Diabetic Medications N/A $20 copay
Mail Order Pharmacy (90-day supply)
Generic $25 copay $25 copay
Brand Preferred $100 copay $100 copay
Brand Non-Preferred $137.50 copay $137.50 copay
Specialty N/A $200 copay
Diabetic Medications N/A $50 copay
2 Amount is prorated for hires after January 1 of plan year.
6