
Page 89 - 2022 Washington Nationals Flipbook
P. 89
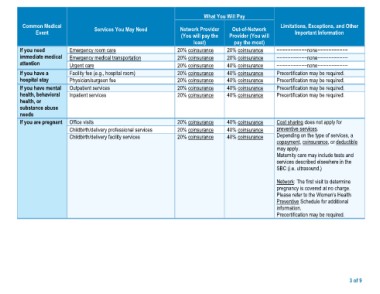
What You Will Pay
Common Medical Services You May Need Network Provider Out-of-Network Limitations, Exceptions, and Other
Event (You will pay the Provider (You will Important Information
If you need Emergency room care least) pay the most) −−−−−−−−−−−none−−−−−−−−−−−
immediate medical Emergency medical transportation −−−−−−−−−−−none−−−−−−−−−−−
attention Urgent care 20% coinsurance 20% coinsurance −−−−−−−−−−−none−−−−−−−−−−−
Facility fee (e.g., hospital room) Precertification may be required.
If you have a Physician/surgeon fee 20% coinsurance 20% coinsurance Precertification may be required.
hospital stay Outpatient services Precertification may be required.
Inpatient services 20% coinsurance 40% coinsurance Precertification may be required.
If you have mental
health, behavioral Office visits 20% coinsurance 40% coinsurance
health, or Childbirth/delivery professional services 20% coinsurance 40% coinsurance
substance abuse Childbirth/delivery facility services
needs 20% coinsurance 40% coinsurance
20% coinsurance 40% coinsurance
If you are pregnant
20% coinsurance 40% coinsurance Cost sharing does not apply for
preventive services.
20% coinsurance 40% coinsurance Depending on the type of services, a
20% coinsurance 40% coinsurance copayment, coinsurance, or deductible
may apply.
Maternity care may include tests and
services described elsewhere in the
SBC (i.e. ultrasound.)
Network: The first visit to determine
pregnancy is covered at no charge.
Please refer to the Women’s Health
Preventive Schedule for additional
information.
Precertification may be required.
3 of 9