
Page 6 - 2023 Microbe Benefit Guide
P. 6
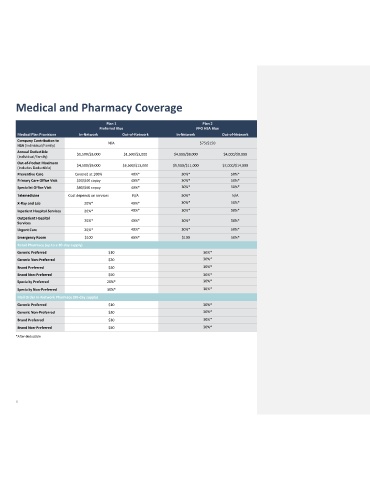
Medical and Pharmacy Coverage
Plan 1 Plan 2
Preferred Blue PPO HSA Blue
Medical Plan Provisions In-Network Out-of-Network In-Network Out-of-Network
Company Contribution to N/A $75/$150
HSA (Individual/Family)
Annual Deductible
$1,500/$3,000 $1,500/$3,000 $4,000/$8,000 $4,000/$8,000
(Individual/Family)
Out-of-Pocket Maximum $4,500/$9,000 $6,500/$13,000 $5,500/$11,000 $7,000/$14,000
(Includes Deductible)
Preventive Care Covered at 100% 40%* 30%* 50%*
Primary Care Office Visit $20/$40 copay 40%* 30%* 50%*
Specialist Office Visit $40/$60 copay 40%* 30%* 50%*
Telemedicine Cost depends on services N/A 30%* N/A
X-Ray and Lab 20%* 40%* 30%* 50%*
Inpatient Hospital Services 20%* 40%* 30%* 50%*
Outpatient Hospital 20%* 40%* 30%* 50%*
Services
Urgent Care 20%* 40%* 30%* 50%*
Emergency Room $100 40%* $100 50%*
Retail Pharmacy (up to a 30-day supply)
Generic Preferred $10 30%*
Generic Non-Preferred $20 30%*
Brand Preferred $30 30%*
Brand Non-Preferred $50 30%*
Specialty Preferred 20%* 30%*
Specialty Non-Preferred 30%* 30%*
Mail Order In-Network Pharmacy (90-day supply)
Generic Preferred $10 30%*
Generic Non-Preferred $20 30%*
Brand Preferred $30 30%*
Brand Non-Preferred $50 30%*
*After deductible
6