
Page 234 - Washington Nationals 2023 Benefits Guide -10.26.22_Neat
P. 234
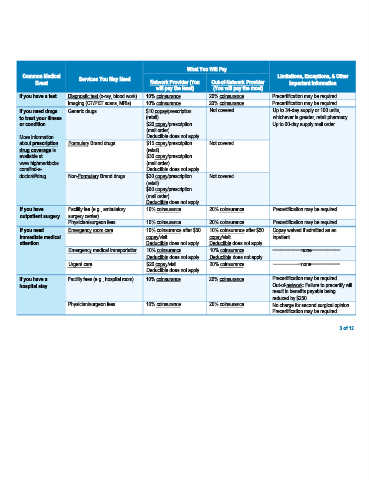
What You Will Pay
Common Medical Services You May Need Limitations, Exceptions, & Other
Event Network Provider (You Out-of-Network Provider Important Information
will pay the least) (You will pay the most)
If you have a test Diagnostic test (x-ray, blood work) 10% coinsurance 20% coinsurance Precertification may be required.
Imaging (CT/PET scans, MRIs) 10% coinsurance 20% coinsurance Precertification may be required.
If you need drugs Generic drugs $10 copay/prescription Not covered Up to 34-day supply or 100 units,
to treat your illness (retail) whichever is greater, retail pharmacy.
or condition $20 copay/prescription Up to 90-day supply mail order.
(mail order)
More information Deductible does not apply.
about prescription Formulary Brand drugs $15 copay/prescription Not covered
drug coverage is (retail)
available at $30 copay/prescription
www.highmarkbcbs. (mail order)
com/find-a- Deductible does not apply.
doctor/#/drug. Non-Formulary Brand drugs $30 copay/prescription Not covered
(retail)
$60 copay/prescription
(mail order)
Deductible does not apply.
If you have Facility fee (e.g., ambulatory 10% coinsurance 20% coinsurance Precertification may be required.
outpatient surgery surgery center)
Physician/surgeon fees 10% coinsurance 20% coinsurance Precertification may be required.
If you need Emergency room care 10% coinsurance after $50 10% coinsurance after $50 Copay waived if admitted as an
immediate medical copay/visit copay/visit inpatient.
attention Deductible does not apply. Deductible does not apply.
Emergency medical transportation 10% coinsurance 10% coinsurance −−−−−−−−−−−none−−−−−−−−−−−
Deductible does not apply. Deductible does not apply.
Urgent care $20 copay/visit 20% coinsurance −−−−−−−−−−−none−−−−−−−−−−−
Deductible does not apply.
If you have a Facility fees (e.g., hospital room) 10% coinsurance 20% coinsurance Precertification may be required.
hospital stay Out-of-network: Failure to precertify will
result in benefits payable being
reduced by $250.
Physician/surgeon fees 10% coinsurance 20% coinsurance No charge for second surgical opinion.
Precertification may be required.
3 of 12