
Page 7 - Tessenderlo Kerley, Inc 2022 Benefit Guide
P. 7
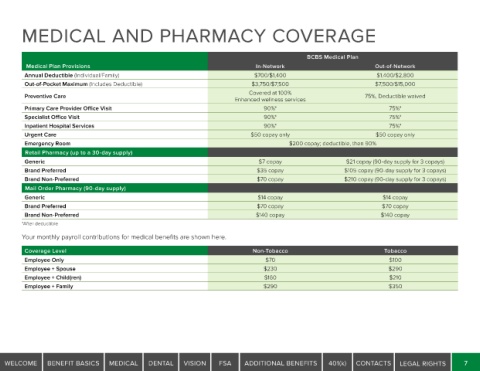
MEDICAL AND PHARMACY COVERAGE
BCBS Medical Plan
Medical Plan Provisions In-Network Out-of-Network
Annual Deductible (Individual/Family) $700/$1,400 $1,400/$2,800
Out-of-Pocket Maximum (Includes Deductible) $3,750/$7,500 $7,500/$15,000
Covered at 100%
Preventive Care 75%, Deductible waived
Enhanced wellness services
Primary Care Provider Office Visit 90%* 75%*
Specialist Office Visit 90%* 75%*
Inpatient Hospital Services 90%* 75%*
Urgent Care $50 copay only $50 copay only
Emergency Room $200 copay; deductible, then 90%
Retail Pharmacy (up to a 30-day supply)
Generic $7 copay $21 copay (90-day supply for 3 copays)
Brand Preferred $35 copay $105 copay (90-day supply for 3 copays)
Brand Non-Preferred $70 copay $210 copay (90-day supply for 3 copays)
Mail Order Pharmacy (90-day supply)
Generic $14 copay $14 copay
Brand Preferred $70 copay $70 copay
Brand Non-Preferred $140 copay $140 copay
*After deductible
Your monthly payroll contributions for medical benefits are shown here.
Coverage Level Non-Tobacco Tobacco
Employee Only $70 $100
Employee + Spouse $230 $290
Employee + Child(ren) $160 $210
Employee + Family $290 $350
WELCOME BENEFIT BASICS MEDICAL DENTAL VISION FSA ADDITIONAL BENEFITS 401(k) CONTACTS LEGAL RIGHTS 7