
Page 8 - 2021 Dreyer's Benefits Guide
P. 8
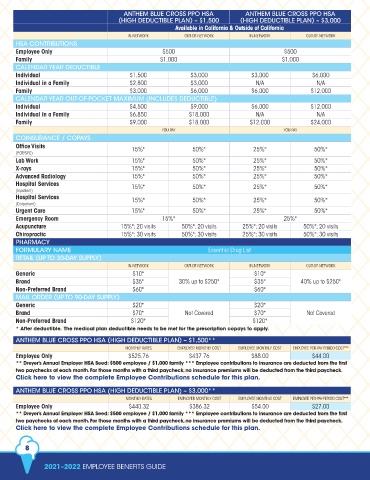
ANTHEM BLUE CROSS PPO HSA ANTHEM BLUE CROSS PPO HSA
(HIGH DEDUCTIBLE PLAN) – $1,500 (HIGH DEDUCTIBLE PLAN) – $3,000
Available in California & Outside of California
IN-NETWORK OUT-OF-NETWORK IN-NETWORK OUT-OF-NETWORK
HSA CONTRIBUTIONS
Employee Only $500 $500
Family $1,000 $1,000
CALENDAR YEAR DEDUCTIBLE
Individual $1,500 $3,000 $3,000 $6,000
Individual in a Family $2,800 $3,000 N/A N/A
Family $3,000 $6,000 $6,000 $12,000
CALENDAR YEAR OUT-OF-POCKET MAXIMUM (INCLUDES DEDUCTIBLE)
Individual $4,500 $9,000 $6,000 $12,000
Individual in a Family $6,850 $18,000 N/A N/A
Family $9,000 $18,000 $12,000 $24,000
YOU PAY YOU PAY
COINSURANCE / COPAYS
Office Visits 15%* 50%* 25%* 50%*
(PCP/SPC)
Lab Work 15%* 50%* 25%* 50%*
X-rays 15%* 50%* 25%* 50%*
Advanced Radiology 15%* 50%* 25%* 50%*
Hospital Services 15%* 50%* 25%* 50%*
(Inpatient)
Hospital Services 15%* 50%* 25%* 50%*
(Outpatient)
Urgent Care 15%* 50%* 25%* 50%*
Emergency Room 15%* 25%*
Acupuncture 15%*; 20 visits 50%*; 20 visits 25%*; 20 visits 50%*; 20 visits
Chiropractic 15%*; 30 visits 50%*; 30 visits 25%*; 30 visits 50%*; 30 visits
PHARMACY
FORMULARY NAME Essential Drug List
RETAIL (UP TO 30-DAY SUPPLY)
IN-NETWORK OUT-OF-NETWORK IN-NETWORK OUT-OF-NETWORK
Generic $10* $10*
Brand $35* 30% up to $250* $35* 40% up to $250*
Non-Preferred Brand $60* $60*
MAIL ORDER (UP TO 90-DAY SUPPLY)
Generic $20* $20*
Brand $70* Not Covered $70* Not Covered
Non-Preferred Brand $120* $120*
* After deductible. The medical plan deductible needs to be met for the prescription copays to apply.
ANTHEM BLUE CROSS PPO HSA (HIGH DEDUCTIBLE PLAN) – $1,500**
MONTHLY RATES EMPLOYER MONTHLY COST EMPLOYEE MONTHLY COST EMPLOYEE PER-PAY-PERIOD COST***
Employee Only $525.76 $437.76 $88.00 $44.00
** Dreyer’s Annual Employer HSA Seed: $500 employee / $1,000 family *** Employee contributions to insurance are deducted from the first
two paychecks of each month. For those months with a third paycheck, no insurance premiums will be deducted from the third paycheck.
Click here to view the complete Employee Contributions schedule for this plan.
ANTHEM BLUE CROSS PPO HSA (HIGH DEDUCTIBLE PLAN) – $3,000**
MONTHLY RATES EMPLOYER MONTHLY COST EMPLOYEE MONTHLY COST EMPLOYEE PER-PAY-PERIOD COST***
Employee Only $440.32 $386.32 $54.00 $27.00
** Dreyer’s Annual Employer HSA Seed: $500 employee / $1,000 family *** Employee contributions to insurance are deducted from the first
two paychecks of each month. For those months with a third paycheck, no insurance premiums will be deducted from the third paycheck.
Click here to view the complete Employee Contributions schedule for this plan.
8
2021–2022 EMPLOYEE BENEFITS GUIDE