
Page 4 - 2024 ANS Benefit Guide
P. 4
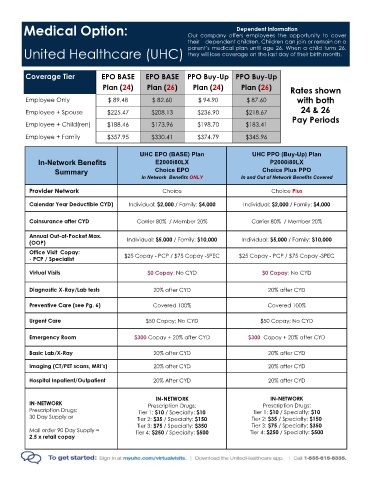
Medical Option: Our company offers employees the opportunity to cover
Dependent Information
their dependent children. Children can join or remain on a
parent’s medical plan until age 26. When a child turns 26,
they will lose coverage on the last day of their birth month.
United Healthcare (UHC)
Coverage Tier EPO BASE EPO BASE PPO Buy-Up PPO Buy-Up
Plan (24) Plan (26) Plan (24) Plan (26) Rates shown
Employee Only $ 89.48 $ 82.60 $ 94.90 $ 87.60 with both
Employee + Spouse $225.47 $208.13 $236.90 $218.67 24 & 26
Pay Periods
Employee + Child(ren) $188.46 $173.96 $198.70 $183.41
Employee + Family $357.95 $330.41 $374.79 $345.96
UHC EPO (BASE) Plan UHC PPO (Buy-Up) Plan
In-Network Benefits E2000i80LX P2000i80LX
Summary Choice EPO Choice Plus PPO
In Network Benefits ONLY In and Out of Network Benefits Covered
Provider Network Choice Choice Plus
Calendar Year Deductible CYD) Individual: $2,000 / Family: $4,000 Individual: $2,000 / Family: $4,000
Coinsurance after CYD Carrier 80% / Member 20% Carrier 80% / Member 20%
Annual Out-of-Pocket Max. Individual: $5,000 / Family: $10,000 Individual: $5,000 / Family: $10,000
(OOP)
Office Visit Copay: $25 Copay - PCP / $75 Copay -SPEC $25 Copay - PCP / $75 Copay -SPEC
- PCP / Specialist
Virtual Visits $0 Copay; No CYD $0 Copay; No CYD
Diagnostic X-Ray/Lab tests 20% after CYD 20% after CYD
Preventive Care (see Pg. 6) Covered 100% Covered 100%
Urgent Care $50 Copay; No CYD $50 Copay; No CYD
Emergency Room $300 Copay + 20% after CYD $300 Copay + 20% after CYD
Basic Lab/X-Ray 20% after CYD 20% after CYD
Imaging (CT/PET scans, MRI’s) 20% after CYD 20% after CYD
Hospital Inpatient/Outpatient 20% After CYD 20% after CYD
IN-NETWORK IN-NETWORK
IN-NETWORK Prescription Drugs: Prescription Drugs:
Prescription Drugs: Tier 1: $10 / Specialty: $10 Tier 1: $10 / Specialty: $10
30 Day Supply or Tier 2: $35 / Specialty: $150 Tier 2: $35 / Specialty: $150
Tier 3: $75 / Specialty: $350 Tier 3: $75 / Specialty: $350
Mail order 90 Day Supply = Tier 4: $250 / Specialty: $500 Tier 4: $250 / Specialty: $500
2.5 x retail copay
4