
Page 4 - Ally Office Solutions - Benefit Guide 2025
P. 4
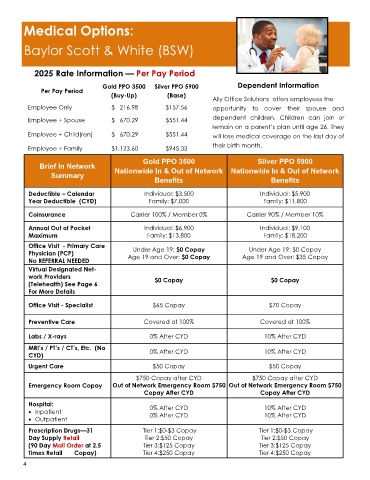
Medical Options:
Baylor Scott & White (BSW)
2025 Rate Information — Per Pay Period
Gold PPO 3500 Silver PPO 5900 Dependent Information
Per Pay Period
(Buy-Up) (Base)
Ally Office Solutions offers employees the
Employee Only $ 216.98 $157.56 opportunity to cover their spouse and
Employee + Spouse $ 670.29 $551.44 dependent children. Children can join or
remain on a parent’s plan until age 26. They
Employee + Child(ren) $ 670.29 $551.44 will lose medical coverage on the last day of
Employee + Family $1,123.60 $945.33 their birth month.
Gold PPO 3500 Silver PPO 5900
Brief In Network
Nationwide In & Out of Network Nationwide In & Out of Network
Summary
Benefits Benefits
Deductible – Calendar Individual: $3,500 Individual: $5,900
Year Deductible (CYD) Family: $7,000 Family: $11,800
Coinsurance Carrier 100% / Member 0% Carrier 90% / Member 10%
Annual Out of Pocket Individual: $6,900 Individual: $9,100
Maximum Family: $13,800 Family: $18,200
Office Visit - Primary Care Under Age 19: $0 Copay Under Age 19: $0 Copay
Physician (PCP) Age 19 and Over: $0 Copay Age 19 and Over: $35 Copay
No REFERRAL NEEDED
Virtual Designated Net-
work Providers $0 Copay $0 Copay
(Telehealth) See Page 6
For More Details
Office Visit - Specialist $65 Copay $70 Copay
Preventive Care Covered at 100% Covered at 100%
Labs / X-rays 0% After CYD 10% After CYD
MRI’s / PT’s / CT’s, Etc. (No 0% After CYD 10% After CYD
CYD)
Urgent Care $50 Copay $50 Copay
$750 Copay after CYD $750 Copay after CYD
Emergency Room Copay Out of Network Emergency Room $750 Out of Network Emergency Room $750
Copay After CYD Copay After CYD
Hospital: 0% After CYD 10% After CYD
• Inpatient 0% After CYD 10% After CYD
• Outpatient
Prescription Drugs—31 Tier 1:$0-$3 Copay Tier 1:$0-$3 Copay
Day Supply Retail Tier 2:$50 Copay Tier 2:$50 Copay
(90 Day Mail Order at 2.5 Tier 3:$125 Copay Tier 3:$125 Copay
Times Retail Copay) Tier 4:$250 Copay Tier 4:$250 Copay
4