
Page 4 - 2025-26 Gas Clip Technologies Benefit Guide2
P. 4
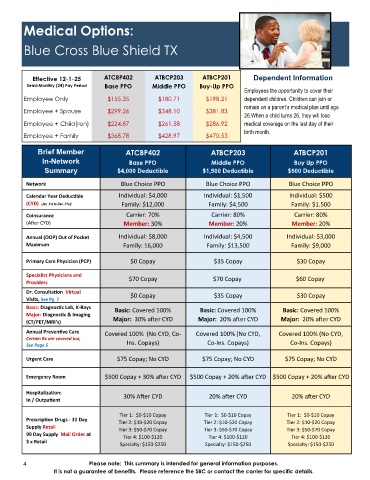
Medical Options:
Blue Cross Blue Shield TX
Effective 12-1-25 ATCBP402 ATBCP203 ATBCP201 Dependent Information
Semi-Monthly (24) Pay Period Base PPO Middle PPO Buy-Up PPO
Employees the opportunity to cover their
Employee Only $155.35 $180.71 $198.21 dependent children. Children can join or
remain on a parent’s medical plan until age
Employee + Spouse $299.26 $348.10 $381.83
26.When a child turns 26, they will lose
Employee + Child(ren) $224.87 $261.58 $286.92 medical coverage on the last day of their
birth month.
Employee + Family $368.78 $428.97 $470.53
Brief Member ATCBP402 ATBCP203 ATBCP201
In-Network Base PPO Middle PPO Buy Up PPO
Summary $4,000 Deductible $1,500 Deductible $500 Deductible
Network Blue Choice PPO Blue Choice PPO Blue Choice PPO
Calendar Year Deductible Individual: $4,000 Individual: $1,500 Individual: $500
Family: $12,000 Family: $4,500 Family: $1.500
(CYD) (Jan .1st to Dec. 31st)
Coinsurance Carrier: 70% Carrier: 80% Carrier: 80%
(After CYD) Member: 30% Member: 20% Member: 20%
Annual (OOP) Out of Pocket Individual: $8,000 Individual: $4,500 Individual: $3,000
Maximum Family: 16,000 Family: $13,500 Family: $9,000
Primary Care Physician (PCP) $0 Copay $35 Copay $30 Copay
Specialist Physicians and $70 Copay $70 Copay $60 Copay
Providers
Dr. Consultation Virtual $0 Copay $35 Copay $30 Copay
Visits, See Pg. 7
Basic: Diagnostic Lab, X-Rays Basic: Covered 100% Basic: Covered 100% Basic: Covered 100%
Major: Diagnostic & Imaging
(CT/PET/MRI’s) Major: 30% after CYD Major: 20% after CYD Major: 20% after CYD
Annual Preventive Care Covered 100% (No CYD, Co- Covered 100% (No CYD, Covered 100% (No CYD,
Certain Rx are covered too,
See Page 5 Ins. Copays) Co-Ins. Copays) Co-Ins. Copays)
Urgent Care $75 Copay; No CYD $75 Copay; No CYD $75 Copay; No CYD
Emergency Room $500 Copay + 30% after CYD $500 Copay + 20% after CYD $500 Copay + 20% after CYD
Hospitalization: 30% After CYD 20% after CYD 20% after CYD
In / Outpatient
Tier 1: $0-$10 Copay Tier 1: $0-$10 Copay Tier 1: $0-$10 Copay
Prescription Drugs - 31 Day
T
Tier 2: $10-$20 Copay
e
i
Tier 2: $10-$20 Copay r 2: $10-$20 Copay
Supply Retail
Tier 3: $50-$70 Copay Tier 3: $50-$70 Copay Tier 3: $50-$70 Copay
90 Day Supply Mail Order at
Tier 4: $100-$120 Tier 4: $100-$120 Tier 4: $100-$120
3 x Retail
Specialty: $150-$250 Specialty: $150-$250 Specialty: $150-$250
4 Please note: This summary is intended for general information purposes.
It is not a guarantee of benefits. Please reference the SBC or contact the carrier for specific details.