
Page 14 - 2025 Texas Flood LLP - Benefit Guide
P. 14
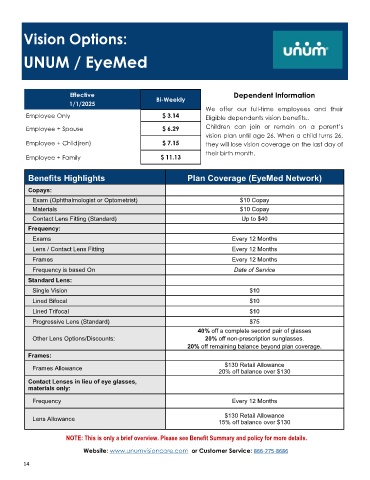
Vision Options:
UNUM / EyeMed
Effective Dependent Information
Bi-Weekly
1/1/2025
We offer our full-time employees and their
Employee Only $ 3.14 Eligible dependents vision benefits..
Employee + Spouse $ 6.29 Children can join or remain on a parent’s
vision plan until age 26. When a child turns 26,
Employee + Child(ren) $ 7.15 they will lose vision coverage on the last day of
their birth month.
Employee + Family $ 11.13
Benefits Highlights Plan Coverage (EyeMed Network)
Copays:
Exam (Ophthalmologist or Optometrist) $10 Copay
Materials $10 Copay
Contact Lens Fitting (Standard) Up to $40
Frequency:
Exams Every 12 Months
Lens / Contact Lens Fitting Every 12 Months
Frames Every 12 Months
Frequency is based On Date of Service
Standard Lens:
Single Vision $10
Lined Bifocal $10
Lined Trifocal $10
Progressive Lens (Standard) $75
40% off a complete second pair of glasses
Other Lens Options/Discounts: 20% off non-prescription sunglasses.
20% off remaining balance beyond plan coverage.
Frames:
$130 Retail Allowance
Frames Allowance
20% off balance over $130
Contact Lenses in lieu of eye glasses,
materials only:
Frequency Every 12 Months
$130 Retail Allowance
Lens Allowance
15% off balance over $130
NOTE: This is only a brief overview. Please see Benefit Summary and policy for more details.
Website: www.unumvisioncare.com or Customer Service: 866-275-8686
14