
Page 4 - Summit LTC Management LLC_Benefit Guide_GROUP 2 2019-2020_Revised 10-1-2020
P. 4
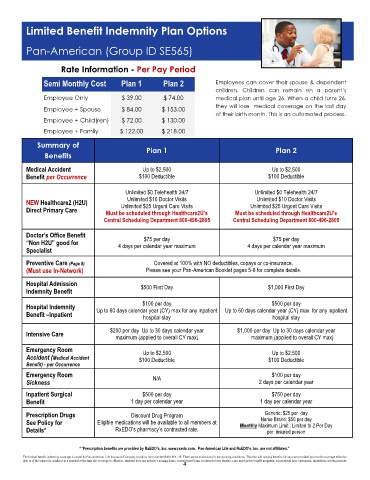
Limited Benefit Indemnity Plan Options
Pan-American (Group ID SE565)
Rate Information - Per Pay Period
Semi Monthly Cost Plan 1 Plan 2 Employees can cover their spouse & dependent
children. Children can remain on a parent’s
Employee Only $ 39.00 $ 74.00 medical plan until age 26. When a child turns 26,
they will lose medical coverage on the last day
Employee + Spouse $ 84.00 $ 153.00
of their birth month. This is an automated process.
Employee + Child(ren) $ 72.00 $ 130.00
Employee + Family $ 122.00 $ 218.00
Summary of Plan 1 Plan 2
Benefits
Medical Accident Up to $2,500 Up to $2,500
Benefit per Occurrence $100 Deductible $100 Deductible
Unlimited $0 Telehealth 24/7 Unlimited $0 Telehealth 24/7
Unlimited $10 Doctor Visits Unlimited $10 Doctor Visits
NEW Healthcare2 (H2U) Unlimited $25 Urgent Care Visits Unlimited $25 Urgent Care Visits
Direct Primary Care Must be scheduled through Healthcare2U’s Must be scheduled through Healthcare2U’s
Central Scheduling Department 800-496-2805 Central Scheduling Department 800-496-2805
Doctor’s Office Benefit $75 per day $75 per day
“Non H2U” good for 4 days per calendar year maximum 4 days per calendar year maximum
Specialist
Preventive Care (Page 8) Covered at 100% with NO deductibles, copays or co-insurance.
(Must use In-Network) Please see your Pan-American Booklet pages 5-8 for complete details.
Hospital Admission $500 First Day $1,000 First Day
Indemnity Benefit
$100 per day $500 per day
Hospital Indemnity Up to 60 days calendar year (CY) max for any inpatient Up to 60 days calendar year (CY) max for any inpatient
Benefit –Inpatient hospital stay hospital stay
$200 per day Up to 30 days calendar year $1,000 per day Up to 30 days calendar year
Intensive Care
maximum (applied to overall CY max) maximum (applied to overall CY max)
Emergency Room Up to $2,500 Up to $2,500
Accident (Medical Accident $100 Deductible $100 Deductible
Benefit) - per Occurrence
Emergency Room N/A $100 per day
Sickness 2 days per calendar year
Inpatient Surgical $500 per day $750 per day
Benefit 1 day per calendar year 1 day per calendar year
Generic: $25 per day
Prescription Drugs Discount Drug Program Name Brand: $50 per day
See Policy for Eligible medications will be available to all members at Monthly Maximum Limit : Limited to 2 Per Day
Details* RxEDO’s pharmacy’s contracted rate. per insured person
*“Prescription benefits are provided by RxEDO's, Inc. www.rxedo.com. Pan-American Life and RxEDO's, Inc. are not affiliated.”
The limited benefit indemnity coverage is issued by Pan-American Life Insurance Company on policy form number PAN-POL-13. There are no exclusions for pre-existing conditions. The plan will not pay benefits for any care provided prior to the coverage effective
date or if the insured is confined in a hospital at the time the coverage is effective. Hospital does not include a nursing home, convalescent home or extended care facility. Like most group benefit programs, our products have exclusions, limitations, waiting periods
4