
Page 4 - National Door_Benefit Guide 2024
P. 4
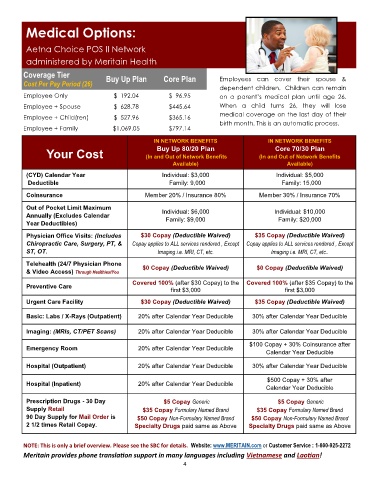
Medical Options:
Aetna Choice POS II Network
administered by Meritain Health
Coverage Tier Buy Up Plan Core Plan
Cost Per Pay Period (26) Employees can cover their spouse &
dependent children. Children can remain
Employee Only $ 192.04 $ 96.95 on a parent’s medical plan until age 26.
Employee + Spouse $ 628.78 $445.64 When a child turns 26, they will lose
Employee + Child(ren) $ 527.96 $365.16 medical coverage on the last day of their
birth month. This is an automatic process.
Employee + Family $1,069.05 $797.14
IN NETWORK BENEFITS IN NETWORK BENEFITS
Buy Up 80/20 Plan
Core 70/30 Plan
Your Cost (In and Out of Network Benefits (In and Out of Network Benefits
Available) Available)
(CYD) Calendar Year Individual: $3,000 Individual: $5,000
Deductible Family: 9,000 Family: 15,000
Coinsurance Member 20% / Insurance 80% Member 30% / Insurance 70%
Out of Pocket Limit Maximum
Annually (Excludes Calendar Individual: $6,000 Individual: $10,000
Year Deductibles) Family: $9,000 Family: $20,000
Physician Office Visits: (Includes $30 Copay (Deductible Waived) $35 Copay (Deductible Waived)
Chiropractic Care, Surgery, PT, & Copay applies to ALL services rendered , Except Copay applies to ALL services rendered , Except
ST, OT. Imaging i.e. MRI, CT, etc. Imaging i.e. MRI, CT, etc..
Telehealth (24/7 Physician Phone $0 Copay (Deductible Waived) $0 Copay (Deductible Waived)
& Video Access) Through HealthiestYou
Covered 100% (after $30 Copay) to the Covered 100% (after $35 Copay) to the
Preventive Care
first $3,000 first $3,000
Urgent Care Facility $30 Copay (Deductible Waived) $35 Copay (Deductible Waived)
Basic: Labs / X-Rays (Outpatient) 20% after Calendar Year Deducible 30% after Calendar Year Deducible
Imaging: (MRIs, CT/PET Scans) 20% after Calendar Year Deducible 30% after Calendar Year Deducible
$100 Copay + 30% Coinsurance after
Emergency Room 20% after Calendar Year Deducible
Calendar Year Deducible
Hospital (Outpatient) 20% after Calendar Year Deducible 30% after Calendar Year Deducible
$500 Copay + 30% after
Hospital (Inpatient) 20% after Calendar Year Deducible
Calendar Year Deducible
Prescription Drugs - 30 Day $5 Copay Generic $5 Copay Generic
Supply Retail $35 Copay Formulary Named Brand 5 Copay Formulary Named Brand
$3
90 Day Supply for Mail Order is $50 Copay Non-Formulary Named Brand 0 Copay Non-Formulary Named Brand
$5
2 1/2 times Retail Copay. Specialty Drugs paid same as Above Specialty Drugs paid same as Above
NOTE: This is only a brief overview. Please see the SBC for details. Website: www.MERITAIN.com or Customer Service : 1-800-925-2272
Meritain provides phone translation support in many languages including Vietnamese and Laotian!
4