
Page 25 - ABC Company 2018 Open Enrollment Guide
P. 25
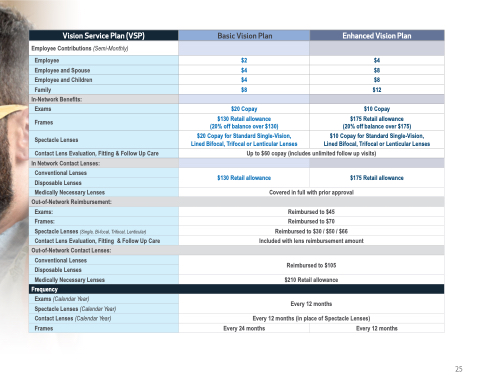
Vision Service Plan (VSP)
Employee and Children
Basic Vision Plan
Enhanced Vision Plan
Employee Contributions (Semi-Monthly)
Employee
$2
$4
Employee and Spouse
$4
$8
$4
$8
Family
$8
$12
In-Network Benefits:
Exams
$20 Copay
$10 Copay
Frames
$130 Retail allowance (20% off balance over $130)
$175 Retail allowance (20% off balance over $175)
Spectacle Lenses
$20 Copay for Standard Single-Vision, Lined Bifocal, Trifocal or Lenticular Lenses
$10 Copay for Standard Single-Vision, Lined Bifocal, Trifocal or Lenticular Lenses
Contact Lens Evaluation, Fitting & Follow Up Care
Up to $60 copay (includes unlimited follow up visits)
In Network Contact Lenses:
Conventional Lenses
Disposable Lenses
$130 Retail allowance
$175 Retail allowance
Medically Necessary Lenses
Covered in full with prior approval
Out-of-Network Reimbursement:
Exams:
Reimbursed to $45
Frames:
Reimbursed to $70
Spectacle Lenses (Single, Bi-focal, Trifocal, Lenticular)
Reimbursed to $30 / $50 / $66
Contact Lens Evaluation, Fitting & Follow Up Care
Included with lens reimbursement amount
Out-of-Network Contact Lenses:
Conventional Lenses
Reimbursed to $105
Disposable Lenses
Medically Necessary Lenses
$210 Retail allowance
Frequency
Exams (Calendar Year)
Spectacle Lenses (Calendar Year)
Contact Lenses (Calendar Year)
Every 12 months
Every 12 months (in place of Spectacle Lenses)
Frames
Every 24 months
Every 12 months
25
