
Page 33 - 2020 Benefit
P. 33
A Guide to Your Health and Wellness Benefits | 2020
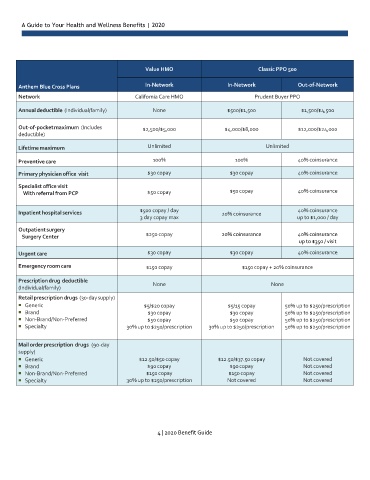
Value HMO Classic PPO 500
Anthem Blue Cross Plans In-Network In-Network Out-of-Network
Network California Care HMO Prudent Buyer PPO
Annual deductible (Individual/family) None $500/$1,500 $1,500/$4,500
Out-of-pocket maximum (Includes $2,500/$5,000 $4,000/$8,000 $12,000/$24,000
deductible)
Lifetime maximum Unlimited Unlimited
Preventive care 100% 100% 40% coinsurance
Primary physician office visit $30 copay $30 copay 40% coinsurance
Specialist office visit
With referral from PCP $50 copay $50 copay 40% coinsurance
$500 copay / day 40% coinsurance
Inpatient hospital services 20% coinsurance
3 day copay max up to $1,000 / day
Outpatient surgery
Surgery Center $250 copay 20% coinsurance 40% coinsurance
up to $350 / visit
Urgent care $30 copay $30 copay 40% coinsurance
Emergency room care $150 copay $150 copay + 20% coinsurance
Prescription drug deductible
None None
(Individual/family)
Retail prescription drugs (30-day supply)
Generic $5/$20 copay $5/15 copay 50% up to $250/prescription
Brand $30 copay $30 copay 50% up to $250/prescription
Non-Brand/Non-Preferred $50 copay $50 copay 50% up to $250/prescription
Specialty 30% up to $250/prescription 30% up to $250/prescription 50% up to $250/prescription
Mail order prescription drugs (90-day
supply)
Generic $12.50/$50 copay $12.50/$37.50 copay Not covered
Brand $90 copay $90 copay Not covered
Non-Brand/Non-Preferred $150 copay $150 copay Not covered
Specialty 30% up to $250/prescription Not covered Not covered
4 | 2020 Benefit Guide