
Page 10 - C:\Users\Ailia\AppData\Local\Temp\msoC899.tmp
P. 10
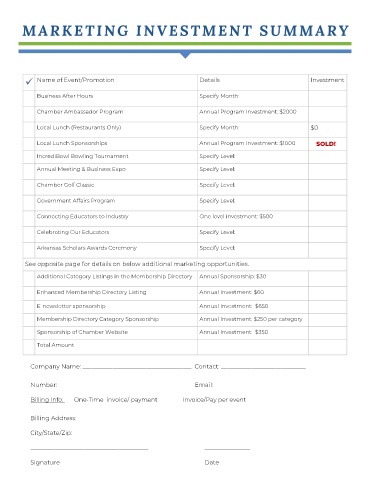
Name of Event/Promotion
ü Details Investment
Business After Hours Specify Month:
Chamber Ambassador Program Annual Program Investment: $2000
Local Lunch (Restaurants Only) Specify Month: $0
Local Lunch Sponsorships Annual Program Investment: $1000 SOLD!
IncrediBowl Bowling Tournament Specify Level:
Annual Meeting & Business Expo Specify Level:
Chamber Golf Classic Specify Level:
Government Affairs Program Specify Level:
Connecting Educators to Industry One level investment: $500
Celebrating Our Educators Specify Level:
Arkansas Scholars Awards Ceremony Specify Level:
See opposite page for details on below additional marketing opportunities.
Additional Category Listings in the Membership Directory Annual Sponsorship: $30
Enhanced Membership Directory Listing Annual Investment: $60
E-newsletter sponsorship Annual Investment: $650
Membership Directory Category Sponsorship Annual Investment: $250 per category
Sponsorship of Chamber Website Annual Investment: $350
Total Amount
Company Name: ____________________________________ Contact: ____________________________
Number: ____________________________________________ Email: ____________________________________
Billing Info: One-Time invoice/ payment Invoice/Pay per event
Billing Address: __________________________________________________________________________________
City/State/Zip: ____________________________________________________________________________________
_______________________________________ _______________
Signature Date