
Page 20 - 2021 Benefits Guide ENGLISH_Flipbook
P. 20
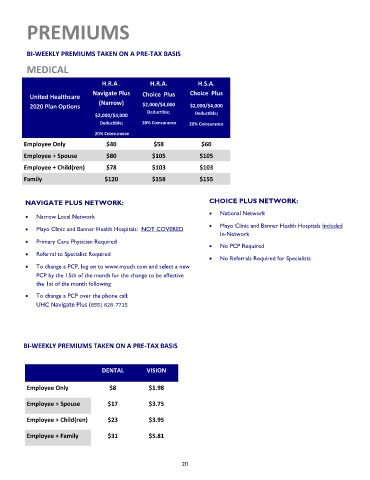
PREMIUMS
BI-WEEKLY PREMIUMS TAKEN ON A PRE-TAX BASIS
MEDICAL
H.R.A . H.R.A. H.S.A.
Navigate Plus Choice Plus Choice Plus
United Healthcare
(Narrow)
2020 Plan Options $2,000/$4,000 $2,000/$4,000
Deductible; Deductible;
$2,000/$4,000
Deductible; 20% Coinsurance 20% Coinsurance
20% Coinsurance
Employee Only $40 $58 $60
Employee + Spouse $80 $105 $105
Employee + Child(ren) $78 $103 $103
Family $120 $158 $155
NAVIGATE PLUS NETWORK: CHOICE PLUS NETWORK:
• National Network
• Narrow Local Network
• Mayo Clinic and Banner Health Hospitals: NOT COVERED • Mayo Clinic and Banner Health Hospitals Included
In-Network
• Primary Care Physician Required
• No PCP Required
• Referral to Specialist Required
• No Referrals Required for Specialists
• To change a PCP, log on to www.myuch.com and select a new
PCP by the 15th of the month for the change to be effective
the 1st of the month following
• To change a PCP over the phone call:
UHC Navigate Plus (855) 828-7715
BI-WEEKLY PREMIUMS TAKEN ON A PRE-TAX BASIS
DENTAL VISION
Employee Only $8 $1.98
Employee + Spouse $17 $3.75
Employee + Child(ren) $23 $3.95
Employee + Family $31 $5.81
20