
Page 12 - VIP Mortgage Benefit Guide FINAL
P. 12
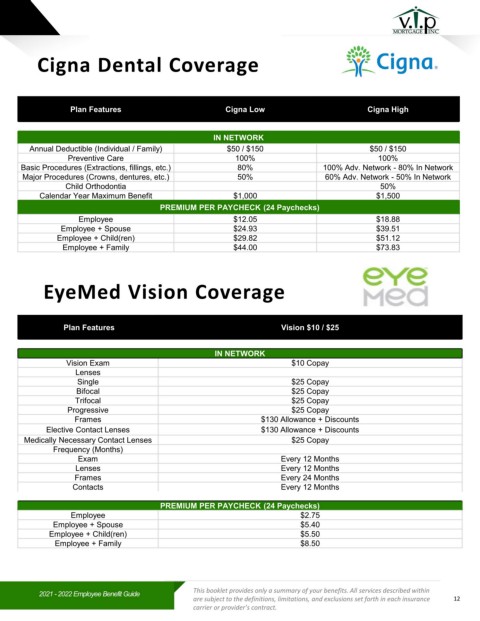
Cigna Dental Coverage
Plan Features Cigna Low Cigna High
IN NETWORK
Annual Deductible (Individual / Family) $50 / $150 $50 / $150
Preventive Care 100% 100%
Basic Procedures (Extractions, fillings, etc.) 80% 100% Adv. Network - 80% In Network
Major Procedures (Crowns, dentures, etc.) 50% 60% Adv. Network - 50% In Network
Child Orthodontia 50%
Calendar Year Maximum Benefit $1,000 $1,500
PREMIUM PER PAYCHECK (24 Paychecks)
Employee $12.05 $18.88
Employee + Spouse $24.93 $39.51
Employee + Child(ren) $29.82 $51.12
Employee + Family $44.00 $73.83
EyeMed Vision Coverage
Plan Features Vision $10 / $25
IN NETWORK
Vision Exam $10 Copay
Lenses
Single $25 Copay
Bifocal $25 Copay
Trifocal $25 Copay
Progressive $25 Copay
Frames $130 Allowance + Discounts
Elective Contact Lenses $130 Allowance + Discounts
Medically Necessary Contact Lenses $25 Copay
Frequency (Months)
Exam Every 12 Months
Lenses Every 12 Months
Frames Every 24 Months
Contacts Every 12 Months
PREMIUM PER PAYCHECK (24 Paychecks)
Employee $2.75
Employee + Spouse $5.40
Employee + Child(ren) $5.50
Employee + Family $8.50
This booklet provides only a summary of your benefits. All services described within
2021 -2022 Employee Benefit Guide
are subject to the definitions, limitations, and exclusions set forth in each insurance 12
carrier or provider’s contract.