
Page 3 - Flyer Employee Benefits Brochure FINAL 2021 OOS w_compliance notices update 3_9
P. 3
Flyer Defense
2021–22 Employee Benefits Brochure
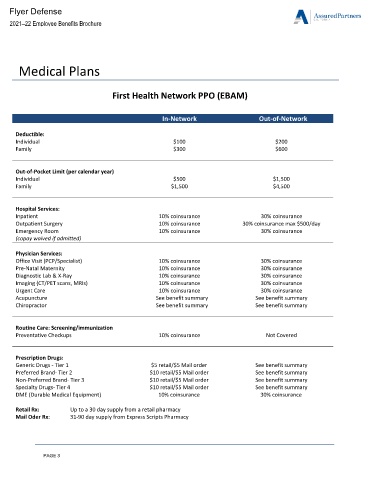
Medical Plans
First Health Network PPO (EBAM)
In-Network Out-of-Network
Deductible:
Individual $100 $200
Family $300 $600
Out-of-Pocket Limit (per calendar year)
Individual $500 $1,500
Family $1,500 $4,500
Hospital Services:
Inpatient 10% coinsurance 30% coinsurance
Outpatient Surgery 10% coinsurance 30% coinsurance max $500/day
Emergency Room 10% coinsurance 30% coinsurance
(copay waived if admitted)
Physician Services:
Office Visit (PCP/Specialist) 10% coinsurance 30% coinsurance
Pre-Natal Maternity 10% coinsurance 30% coinsurance
Diagnostic Lab & X-Ray 10% coinsurance 30% coinsurance
Imaging (CT/PET scans, MRIs) 10% coinsurance 30% coinsurance
Urgent Care 10% coinsurance 30% coinsurance
Acupuncture See benefit summary See benefit summary
Chiropractor See benefit summary See benefit summary
Routine Care: Screening/immunization
Preventative Checkups 10% coinsurance Not Covered
Prescription Drugs:
Generic Drugs - Tier 1 $5 retail/$5 Mail order See benefit summary
Preferred Brand- Tier 2 $10 retail/$5 Mail order See benefit summary
Non-Preferred Brand- Tier 3 $10 retail/$5 Mail order See benefit summary
Specialty Drugs- Tier 4 $10 retail/$5 Mail order See benefit summary
DME (Durable Medical Equipment) 10% coinsurance 30% coinsurance
Retail Rx: Up to a 30 day supply from a retail pharmacy
Mail Oder Rx: 31-90 day supply from Express Scripts Pharmacy
PAGE 3