
Page 5 - Artemis 2021 Employee Benefits
P. 5
Artemis Health
2021 Employee Benefits Brochure
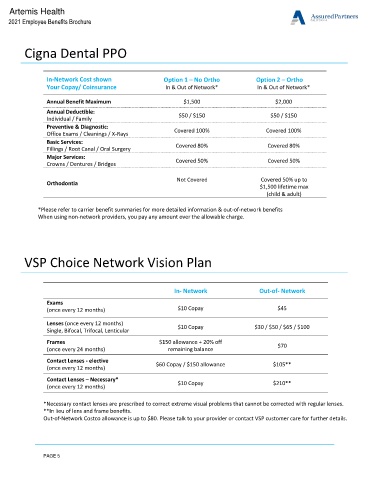
Cigna Dental PPO
In-Network Cost shown Option 1 – No Ortho Option 2 – Ortho
Your Copay/ Coinsurance In & Out of Network* In & Out of Network*
Annual Benefit Maximum $1,500 $2,000
Annual Deductible:
Individual / Family $50 / $150 $50 / $150
Preventive & Diagnostic:
Office Exams / Cleanings / X-Rays Covered 100% Covered 100%
Basic Services:
Fillings / Root Canal / Oral Surgery Covered 80% Covered 80%
Major Services:
Crowns / Dentures / Bridges Covered 50% Covered 50%
Not Covered Covered 50% up to
Orthodontia
$1,500 lifetime max
(child & adult)
*Please refer to carrier benefit summaries for more detailed information & out-of-network benefits
When using non-network providers, you pay any amount over the allowable charge.
VSP Choice Network Vision Plan
In- Network Out-of- Network
Exams
(once every 12 months) $10 Copay $45
Lenses (once every 12 months) $10 Copay $30 / $50 / $65 / $100
Single, Bifocal, Trifocal, Lenticular
Frames $150 allowance + 20% off $70
(once every 24 months) remaining balance
Contact Lenses - elective
$60 Copay / $150 allowance $105**
(once every 12 months)
Contact Lenses – Necessary*
$10 Copay $210**
(once every 12 months)
*Necessary contact lenses are prescribed to correct extreme visual problems that cannot be corrected with regular lenses.
**In lieu of lens and frame benefits.
Out-of-Network Costco allowance is up to $80. Please talk to your provider or contact VSP customer care for further details.
PAGE 5