
Page 11 - HBC 2017 - Final
P. 11
International Orthopaedics (SICOT) (2008) 32:115–119 117
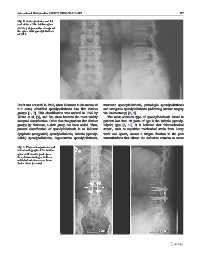
Fig. 2 Anteroposterior and lat-
eral views of the lumbar spine
showing degenerative change of
the spine with spondylolisthesis
of L3-4
But it was not until in 1963, when Newman in his review of traumatic spondylolisthesis, pathologic spondylolisthesis
319 cases, classified spondylolisthesis into five distinct and iatrogenic spondylolisthesis (following lumbar surgery
groups [1, 7]. This classification was revised in 1976 by via laminectomy) [8, 9].
Wiltse et al. [9], and has since become the most widely The most common type of spondylolisthesis found in
accepted classification. Other than the previous five distinct patients less than 50 years of age is the isthmic (spondy-
groups by Newman, a sixth group has been added. Thus, lolytic) type [5, 10]. It is believed that “biomechanical
present classification of spondylolisthesis is as follows: stress”, such as repetitive mechanical strain from heavy
dysplastic (congenital) spondylolisthesis, isthmic (spondy- work and sports, causes a fatigue fracture to the pars
lolitic) spondylolisthesis, degenerative spondylolisthesis, interarticularis that allows the defective vertebra to move
Fig. 3 Plain anteroposterior and
lateral radiograph of the lumbar
spine at 8 months post-opera-
tion, demonstrating a well-con-
solidated intertransverse bone
fusion mass (arrows)