
Page 10 - Sample EE Benefits Guide
P. 10
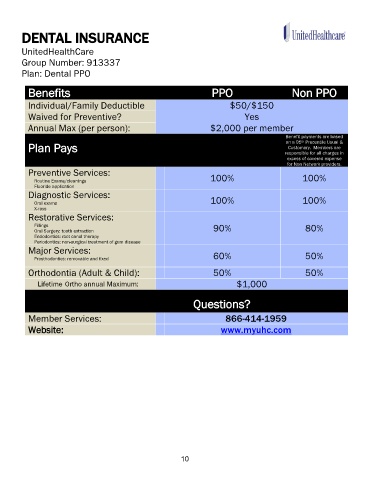
DENTAL INSURANCE
UnitedHealthCare
Group Number: 913337
Plan: Dental PPO
Benefits PPO Non PPO
Individual/Family Deductible $50/$150
Waived for Preventive? Yes
Annual Max (per person): $2,000 per member
Benefit payments are based
on a 95 Precentile Usual &
th
Plan Pays responsible for all charges in
Customary. Members are
excess of covered expense
for Non Network providers.
Preventive Services:
Routine Exams/cleanings 100% 100%
Fluoride application
Diagnostic Services:
Oral exams 100% 100%
X-rays
Restorative Services:
Fillings 90% 80%
Oral Surgery: tooth extraction
Endodontics: root canal therapy
Periodontics: non-surgical treatment of gum disease
Major Services:
Prosthodontics: removable and fixed 60% 50%
Orthodontia (Adult & Child): 50% 50%
Lifetime Ortho annual Maximum: $1,000
Questions?
Member Services: 866-414-1959
Website: www.myuhc.com
10