
Page 69 - NAME OF CONDITION: REFRACTIVE ERRORS
P. 69
associated risk factors is essential. Waiting for the diabetic to present with visual
problems is not a good strategy. Many patients retain normal eyesight or experience
a minimal (and sometimes unnoticeable) reduction of vision even in the presence of
sight-threatening disease (diabetic maculopathy, proliferative disease). It is for this
reason that screening for DR is mandatory. Sometimes, the patients may become
aware of a problem (whether or not they are known diabetics) as in :
A painless gradual reduction of central vision may be associated with any of the
types of DR. The most common cause is diabetic macular oedema. Painless and
gradual visual loss is also associated with coexistent cataract formation
(diabetic or otherwise).
Haemorrhages result in the sudden onset of dark, painless floaters which may
resolve over several days.
Severe vitreous haemorrhage may obscure the vitreous altogether resulting in
a painless visual loss.
An acute attack of glaucoma precipitated by rubeosis iridis is the one situation
where the patient will present with acute pain; urgent referral is essential.
Examination: a complete and comprehensive examination using a direct
ophthalmoscope, indirect ophthalmoscope and slit lamp with 90 dioptre lens is
essential for diagnosing and staging diabetic retinopathy. Careful staging and
appropriate management goes a long way in preventing visual loss due to diabetic
retinopathy.
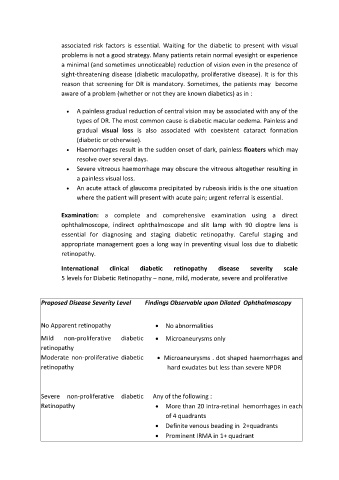
International clinical diabetic retinopathy disease severity scale
5 levels for Diabetic Retinopathy – none, mild, moderate, severe and proliferative
Proposed Disease Severity Level Findings Observable upon Dilated Ophthalmoscopy
No Apparent retinopathy No abnormalities
Mild non-proliferative diabetic Microaneurysms only
retinopathy
Moderate non-proliferative diabetic Microaneurysms . dot shaped haemorrhages and
retinopathy hard exudates but less than severe NPDR
Severe non-proliferative diabetic Any of the following :
Retinopathy More than 20 intra-retinal hemorrhages in each
of 4 quadrants
Definite venous beading in 2+quadrants
Prominent IRMA in 1+ quadrant
69