
Page 4 - Michigan Fitness Foundation 2021 Booklet
P. 4
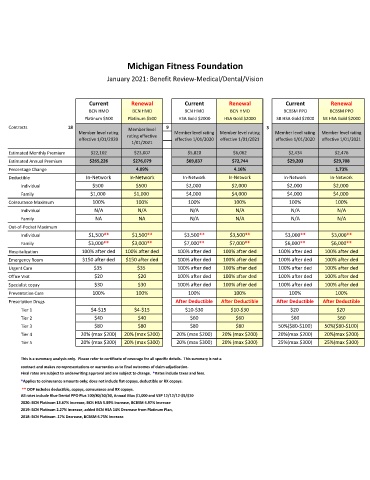
Michigan Fitness Foundation
January 2021: Benefit Review-Medical/Dental/Vision
Current Renewal Current Renewal Current Renewal
BCN HMO BCN HMO BCN HMO BCN HMO BCBSM PPO BCBSM PPO
Platinum $500 Platinum $500 HSA Gold $2000 HSA Gold $2000 SB HSA Gold $2000 SB HSA Gold $2000
Contracts 18 Member level 9 3
Member level rating Member level rating Member level rating Member level rating Member level rating
effective 1/01/2020 rating effective effective 1/01/2020 effective 1/01/2021 effective 1/01/2020 effective 1/01/2021
1/01/2021
Estimated Monthly Premium $22,102 $23,007 $5,820 $6,062 $2,434 $2,476
Estimated Annual Premium $265,226 $276,079 $69,837 $72,744 $29,203 $29,708
Percentage Change 4.09% 4.16% 1.73%
Deductible In-Network In-Network In-Network In-Network In-Network In-Network
Individual $500 $500 $2,000 $2,000 $2,000 $2,000
Family $1,000 $1,000 $4,000 $4,000 $4,000 $4,000
Coinsurance Maximum 100% 100% 100% 100% 100% 100%
Individual N/A N/A N/A N/A N/A N/A
Family NA NA N/A N/A N/A N/A
Out-of-Pocket Maximum
Individual $1,500** $1,500** $3,500** $3,500** $3,000** $3,000**
Family $3,000** $3,000** $7,000** $7,000** $6,000** $6,000**
Hospitalization 100% after ded 100% after ded 100% after ded 100% after ded 100% after ded 100% after ded
Emergency Room $150 after ded $150 after ded 100% after ded 100% after ded 100% after ded 100% after ded
Urgent Care $35 $35 100% after ded 100% after ded 100% after ded 100% after ded
Office Visit $20 $20 100% after ded 100% after ded 100% after ded 100% after ded
Specialist copay $30 $30 100% after ded 100% after ded 100% after ded 100% after ded
Preventative Care 100% 100% 100% 100% 100% 100%
Prescription Drugs After Deductible After Deductible After Deductible After Deductible
Tier 1 $4-$15 $4-$15 $10-$30 $10-$30 $20 $20
Tier 2 $40 $40 $60 $60 $60 $60
Tier 3 $80 $80 $80 $80 50%($80-$100) 50%($80-$100)
Tier 4 20% (max $200) 20% (max $200) 20% (max $200) 20% (max $200) 20%(max $200) 20%(max $200)
Tier 5 20% (max $300) 20% (max $300) 20% (max $300) 20% (max $300) 25%(max $300) 25%(max $300)
This is a summary analysis only. Please refer to certificate of coverage for all specific details. This summary is not a
contract and makes no representations or warranties as to final outcomes of claim adjudication.
Final rates are subject to underwriting approval and are subject to change. *Rates include taxes and fees.
*Applies to coinsurance amounts only; does not include flat copays, deductible or RX copays.
** OOP includes deductible, copays, coinsurance and RX copays.
All rates include Blue Dental PPO Plus 100/80/50/50, Annual Max $1,000 and VSP 12/12/12-$5/$10
2020: BCN Platinum 13.67% increase, BCN HSA 5.89% Increase, BCBSM 4.97% Increase
2019: BCN Platinum 2.27% increase, added BCN HSA 14% Decrease from Platinum Plan,
2018: BCN Platinum .17% Decrease, BCBSM 6.75% Increase