
Page 6 - Michigan Fitness Foundation 2021 Booklet
P. 6
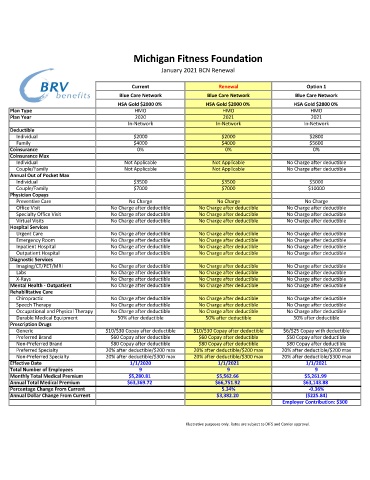
Michigan Fitness Foundation
January 2021 BCN Renewal
Current Renewal Option 1
Blue Care Network Blue Care Network Blue Care Network
HSA Gold $2000 0% HSA Gold $2000 0% HSA Gold $2800 0%
Plan Type HMO HMO HMO
Plan Year 2020 2021 2021
In-Network In-Network In-Network
Deductible
Individual $2000 $2000 $2800
Family $4000 $4000 $5600
Coinsurance 0% 0% 0%
Coinsurance Max
Individual Not Applicable Not Applicable No Charge after deductible
Couple/Family Not Applicable Not Applicable No Charge after deductible
Annual Out of Pocket Max
Individual $3500 $3500 $5000
Couple/Family $7000 $7000 $10000
Physician Copays
Preventive Care No Charge No Charge No Charge
Office Visit No Charge after deductible No Charge after deductible No Charge after deductible
Specialty Office Visit No Charge after deductible No Charge after deductible No Charge after deductible
Virtual Visits No Charge after deductible No Charge after deductible No Charge after deductible
Hospital Services
Urgent Care No Charge after deductible No Charge after deductible No Charge after deductible
Emergency Room No Charge after deductible No Charge after deductible No Charge after deductible
Inpatient Hospital No Charge after deductible No Charge after deductible No Charge after deductible
Outpatient Hospital No Charge after deductible No Charge after deductible No Charge after deductible
Diagnostic Services
Imaging/CT/PET/MRI No Charge after deductible No Charge after deductible No Charge after deductible
Labs No Charge after deductible No Charge after deductible No Charge after deductible
X-Rays No Charge after deductible No Charge after deductible No Charge after deductible
Mental Health - Outpatient No Charge after deductible No Charge after deductible No Charge after deductible
Rehabilitative Care
Chiropractic No Charge after deductible No Charge after deductible No Charge after deductible
Speech Therapy No Charge after deductible No Charge after deductible No Charge after deductible
Occupational and Physical Therapy No Charge after deductible No Charge after deductible No Charge after deductible
Durable Medical Equipment 50% after deductible 50% after deductible 50% after deductible
Prescription Drugs
Generic $10/$30 Copay after deductible $10/$30 Copay after deductible $6/$25 Copay with deductible
Preferred Brand $60 Copay after deductible $60 Copay after deductible $50 Copay after deductible
Non-Preferred Brand $80 Copay after deductible $80 Copay after deductible $80 Copay after deductible
Preferred Specialty 20% after deductible/$200 max 20% after deductible/$200 max 20% after deductible/$200 max
Non-Preferred Specialty 20% after deductible/$300 max 20% after deductible/$300 max 20% after deductible/$300 max
Effective Date 1/1/2020 1/1/2021 1/1/2021
Total Number of Employees 9 9 9
Monthly Total Medical Premium $5,280.81 $5,562.66 $5,261.99
Annual Total Medical Premium $63,369.72 $66,751.92 $63,143.88
Percentage Change From Current 5.34% -0.36%
Annual Dollar Change From Current $3,382.20 ($225.84)
Employer Contribution: $300
Illustrative purposes only. Rates are subject to DIFS and Carrier approval.