
Page 5 - Food Bank Council 2020 Renewal Booklet
P. 5
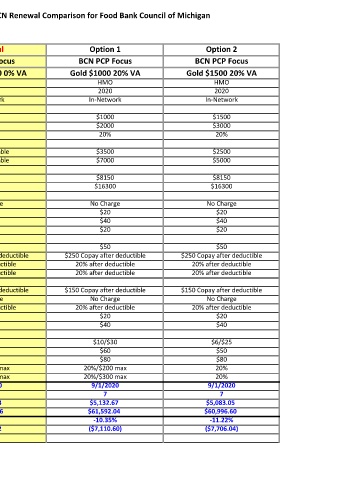
September 2020 BCN Renewal Comparison for Food Bank Council of Michigan
Current Renewal Option 1 Option 2
BCN PCP Focus BCN PCP Focus BCN PCP Focus BCN PCP Focus
Platinum $500 0% VA Platinum $500 0% VA Gold $1000 20% VA Gold $1500 20% VA
Plan Type HMO HMO HMO HMO
Plan Year 2019 2020 2020 2020
In-Network In-Network In-Network In-Network
Deductible
Individual $500 $500 $1000 $1500
Couple/Family $1,000 $1000 $2000 $3000
Coinsurance 0% 0% 20% 20%
Coinsurance Max
Individual N/A Not Applicable $3500 $2500
Couple/Family N/A Not Applicable $7000 $5000
Annual Out of Pocket Max
Individual $1,500 $1500 $8150 $8150
Couple/Family $3,000 $3000 $16300 $16300
Physician Copays
Preventive Care Covered 100% No Charge No Charge No Charge
Office Visit $20 $20 $20 $20
Specialty Office Visit $30 $30 $40 $40
Virtual Visits $20 $20 $20 $20
Hospital Services
Urgent Care $35 $35 $50 $50
Emergency Room $150 after deductible $150 Copay after deductible $250 Copay after deductible $250 Copay after deductible
Inpatient Hospital 0% after dedutible 0% after deductible 20% after deductible 20% after deductible
Outpatient Hospital 0% after dedutible 0% after deductible 20% after deductible 20% after deductible
Diagnostic Services
Imaging/CT/PET/MRI $150 after deductible $150 Copay after deductible $150 Copay after deductible $150 Copay after deductible
Labs 0% after dedutible No Charge No Charge No Charge
X-Rays 0% after dedutible 0% after deductible 20% after deductible 20% after deductible
Mental Health $20 $20 $20 $20
Chiropractic $30 $30 $40 $40
Prescription Drugs
Generic $4/$15 $4/$15 $10/$30 $6/$25
Preferred Brand $40 $40 $60 $50
Non-Preferred Brand $80 $80 $80 $80
Preferred Specialty 20%/$200 max 20%/$200 max 20%/$200 max 20%
Non-Preferred Specialty 20%/$300 max 20%/$300 max 20%/$300 max 20%
Effective Date 9/1/2019 9/1/2020 9/1/2020 9/1/2020
Total Number of Employees 7 7 7 7
Monthly Total Medical Premium $5,725.22 $6,166.43 $5,132.67 $5,083.05
Annual Total Medical Premium $68,702.64 $73,997.16 $61,592.04 $60,996.60
Percentage Change From Current 7.71% -10.35% -11.22%
Annual Dollar Change From Current $5,294.52 ($7,110.60) ($7,706.04)